University of Maryland Medical Center
Baltimore, MD
Program Director: Nirav G. Shah, MD
Type of Program: Pulmonary and Critical Care Medicine
Abstract Authors: Van K. Holden, MD; Avelino C. Verceles, MD, MS; Nirav G. Shah; Michael T. McCurdy, MD; and Kathryn S. Robinett, MD
RATIONALE
Although triaging for ICU admission is a component of many critical care fellowship programs, there have been no studies evaluating the effectiveness of ICU triage education on fellows. Pulmonary/critical care and critical care fellows triage admissions to the MICU at the University of Maryland, a large tertiary care center with a 29-bed closed MICU. Our hypothesis is that a structured triaging orientation program will improve fellows’ comfort level with MICU triaging.
METHODS
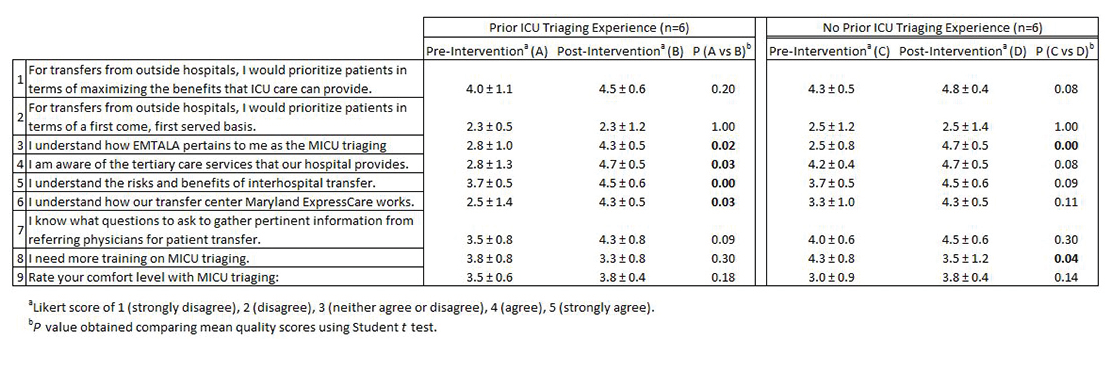
Thirteen entering pulmonary/critical care and critical care fellows attended an hour-long triaging orientation program. The training session included (1) key points of the SCCM Consensus Statement on the Triage of Critically Ill Patients, (2) information on Emergency Medical Treatment & Labor Act (EMTALA), (3) reasons for interhospital transfer, (4) benefits and risks of interhospital transfer, and (5) outcomes of ICU admission delay and refusal. These components were based on a review of the available literature. The second element of the training session addressed institution specific resources, (1) the interhospital transfer process including transport, (2) triaging flow sheet based on bed availability and patient location, and (3) a modified patient transfer accept instrument. The fellows completed a 9-question survey assessing their understanding of these components prior to, and immediately after the training session. Responses were based on a 5-point Likert scale.
RESULTS
Twelve fellows participated in the surveys. Pre- and post-intervention survey responses were compared. Six fellows had prior ICU triaging experience, ranging from 2 to 24 months. The remaining six fellows had no prior ICU triaging experience. After the training session, fellows with prior experience demonstrated a statistically significant increased understanding of EMTALA, tertiary care services that the hospital provided, risks and benefits of interhospital transfer, and how the interhospital transfer process works compared to those without prior experience. This improved understanding persisted when the fellows’ responses were compared based on post-graduate training year 4 vs. 5 and above. Although there was no difference in comfort level with MICU triaging, fellows without prior triaging experience wanted additional training after the intervention. All fellows demonstrated increased knowledge on EMTALA.
CONCLUSION
Our study highlights the finding that fellows with prior ICU triaging experience, or advanced level of post-graduate training, have greater understanding of various components involved in triage decision-making with a structured training session. This suggests that continued training on triaging would be beneficial as part of a critical care fellowship curriculum, regardless of prior experience.