Perelman School of Medicine, University of Pennsylvania
Philadelphia, PA
Program Director: Maryl Krieder
Program Associate Director: Meeta Kerlin
Program Type: Pulmonary/Critical Care
Abstract Authors: Kunal P. Patel*, Janae K. Heath*, Meeta Kerlin, Oana Tomescu, and Maryl Kreider
Description of Fellowship Program: Our fellowship program is a 3.5-year training program in a large urban setting, with six fellows annually. It consists of a total of 18 months of inpatient clinical responsibilities varied between a large tertiary medical center, a community hospital, and a VA hospital. The remaining 24 months consist of ongoing continuity outpatient experiences and additional research training, in areas of clinical research, basic science research, or medical education scholarship.
Abstract
Rationale
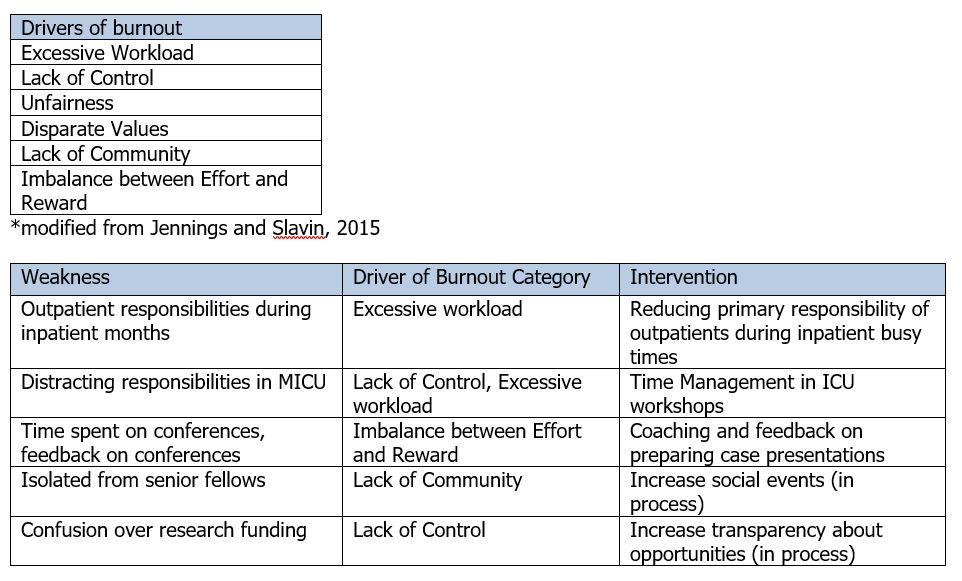
Burnout is an increasingly recognized problem amongst physicians. Unaddressed, burnout can lead to significant health consequences for medical providers and impact the quality of health care delivered. Causes of burnout are multifactorial (table 1) and pulmonary and critical care medicine physicians are at risk because of the intensity and stress inherent to both specialties. Identifying specific drivers of burnout during training could allow programs to innovate ways to reduce structural program components that contribute to burnout and build curriculum about emotional intelligence and resiliency. Given the diversity of programs and trainees, individualizing interventions at a programmatic level likely will be needed and requires a systemic assessment of drivers of burnout. To our knowledge, no standardized approach to address burnout in pulmonary and critical care training programs has previously been described.
Educational Strategy
We used a mixed methods approach to assess our trainees’ levels of burnout and resiliency. First, we administered validated questionnaires to measure burnout (Maslach Burnout Inventory) and resiliency (Connor Davidson Resilience Scale) to all fellows in June 2017. Second, we convened focus groups facilitated by a trained faculty member from outside of our division to obtain unbiased narratives on contributors to burnout and aspects of our training program that were supportive of wellness. Focus groups were conducted separately with first-year and senior fellows given the discordance in clinical responsibilities between those cohorts. Questionnaire results were also reported by year of training. We then engaged fellows to develop interventions that targeted the structural drivers of burnout that were identified in the program-wide assessment. Additionally, lectures focused on wellness and burnout were given to both division faculty and trainees to improve collective knowledge base.
Implementation
All nineteen fellows in our program completed questionnaires. Four of six first-year fellows (66%) had high levels of clinical emotional exhaustion and depersonalization, which are markers of burnout. In contrast, only two of thirteen senior fellows (15%) had high levels of emotional exhaustion and three of thirteen (23%) had high levels of depersonalization. All senior fellows participate in independent research projects and five of seven third year fellows (72%) had a high level emotional exhaustion linked to their research suggesting a high level of a different type of burnout. Resiliency was low across all three years with 66%, 50%, and 57% of fellows scoring as low resiliency in first, second, and third years, respectively. Eleven fellows participated in focus groups (6 first years, 6 second years, 7 third years). Focus group sessions identified several specific areas for improvement (Table 2) as well as areas of strength. Interventions that have since been implemented include (1) reduction of primary responsibility of the care of outpatients during the first year, when inpatient responsibilities are heaviest; (2) development of workshops to teach time management in the ICU, and (3) development of a program of coaching and feedback for preparing expected case presentations to reduce workload and increase educational yield. We plan to repeat assessment at regular intervals including administering the questionnaires every 6 months and focus groups every 12 months with the intention to create an iterative process to continue to assess needs and further improve.
Conclusion
Burnout is a significant issue that is being increasingly recognized and has significant implications for our field. A structured assessment of trainees in our program demonstrated high levels of different types of burnout and led to interventions which we think will improve burnout and build resiliency in our program. Through validated questionnaires and focus groups, we have created a structure to allow for iterative improvement and the process should be transferable to other programs although specific interventions will likely vary.