Reviewed By Critical Care Assembly
Submitted by
David A. Kaufman
Assistant Professor
Mount Sinai School of Medicine
New York, NY
Shawn Knapik
Department of Veterans Affairs
New York Harbor Healthcare System
Brooklyn, NY
Submit your comments to the author(s).
History
A man in his eighth decade presented to his primary doctor three weeks prior to admission with easy bruising. A complete blood count revealed low counts in all three major cell lines and a subsequent bone marrow biopsy demonstrated B-cell follicular lymphoma. Other biochemical parameters, including tests of liver transaminases and bilirubin, were normal. Two weeks later he developed a cough and shortness of breath and he received a diagnosis of “acute bronchitis,” for which he was prescribed azithromycin along with an inhaler of salmeterol and fluticasone.
His cough and dyspnea did not improve and he was admitted to another hospital for further evaluation. A diagnosis of liver failure was made based on elevated liver function tests (aspartate aminotransferase=995 U/L, alanine aminotransferase=552 U/L, total bilirubin=7.2 mg/dL, direct bilirubin=5.5 mg/dL); worsening pancytopenia was noted. Evaluation of the acute liver failure did not reveal an etiology, and he was transferred to a tertiary care hospital for further evaluation and care.
Past Medical & Surgical History:
Thyroid cancer, s/p partial thyroidectomy
Hypothyroidism
Diabetes Mellitus, type 2
Benign prostatic hypertrophy
Medications:
Levothyroxine
Herbal medicines:
- saw palmetto
- milk thistle
- chromium picolinate
Social History:
Denies excessive alcohol and illicit drug use
40 pack-year cigarette smoking history, stopped in 2004
Worked as a welder, retired for 15 years
Married, three adult children
Hospital Course:
Laboratory investigation did not reveal occult infectious hepatitis or autoimmune disease. Diagnostic imaging of the liver revealed a large intra-hepatic mass and trans-jugular liver biopsy showed extensive hepatic infiltration by lymphoma.
His respiratory status became increasingly tenuous and his trachea was intubated and positive-pressure mechanical ventilation was initiated. He was transferred to the ICU but suffered the rapid onset of shock despite infusions of sodium bicarbonate and norepinephrine. After a conversation with his family about his wishes for end-of-life care, further attempts at resuscitation were deferred and the emphasis of care was placed on the amelioration of pain and suffering. He died one day later with his family at his bedside.
Physical Exam
On admission to the Intensive Care Unit:
T=37.3ºC P=93/min BP=134/61 mmHg RR=26/min
SaO2=98% on ambient air
General: alert but moderate respiratory distress, able to hold a conversation despite labored breathing
Head/neck: jaundiced sclerae bilaterally; jugular venous pressure estimated to be normal
Chest: 3+ use of accessory muscles of breathing, clear breath sounds throughout
Cardiac: regular rhythm, no extrasystolic sounds
Abdomen: soft no distension, moderate RUQ tenderness, marked hepatomegaly and splenomegaly
Extremities: warm, strong pulses in all limbs, no edema
Neurologic exam: +asterixis, normal speech pattern and content
Lab
Potassium 4.7 mmol/L
Chloride 106 mmol/L
Bicarbonate 6 mmol /L
Blood urea nitrogen 29 mg/dL
Creatinine 0.3 mg/dL
Glucose 73 mg/dL
Arterial pH 7.05
Arterial PCO2 19 mm Hg
Arterial PO2 140 mm Hg
Arterial lactate 20 mg/dL
Leukocytes 1.4 x103/mm3
Hemoglobin 8.3 g/dL
Platelets 56 x103/mm3
Albumin 1.7 g/dL
Total bilirubin 18.8 mg/dL
Direct (Conjugated) bilirubin 17.8 mg/dL
Aspartate aminotransferase (AST) 997 U/L
Alanine aminotransferase 835 U/L
Lactate dehydrogenase (LDH) 327 U/L
Prothrombin time (PT) 36 sec
International normalized ratio (INR) 2.9
Partial thromboplastin time (PTT) 36.5 sec
Figures
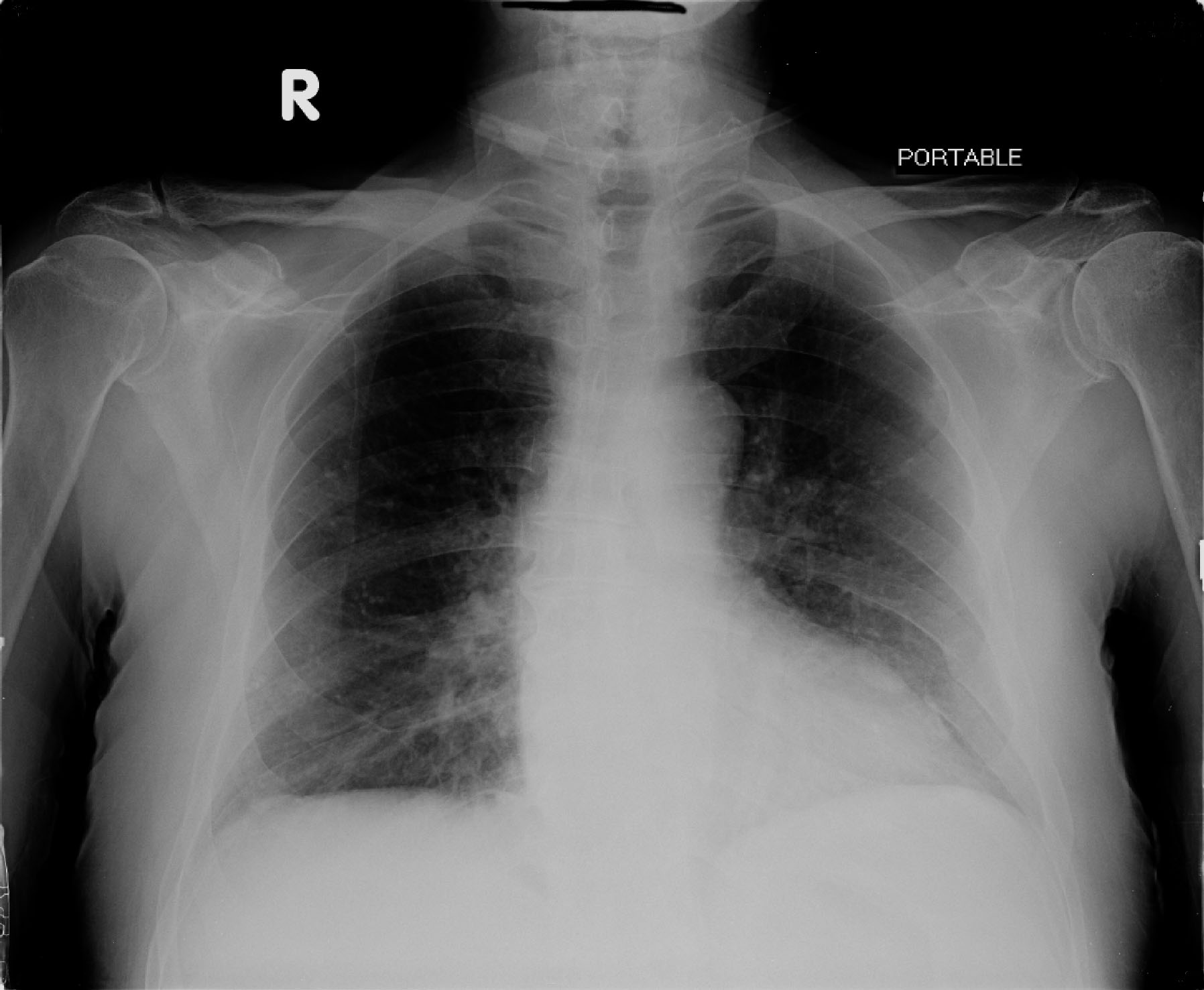
Portable A-P chest radiograph taken on transfer to the tertiary hospital
References
- Gutierrez G, Wulf ME. Lactic acidosis in sepsis: another commentary. Crit Care Med 2005;33(10):2420-2.
- Prikis M, Mesler EL, Hood VL, Weise WJ. When a friend can become an enemy! Recognition and management of metformin-associated lactic acidosis. Kidney Int 2007.
- Sillos EM, Shenep JL, Burghen GA, Pui CH, Behm FG, Sandlund JT. Lactic acidosis: a metabolic complication of hematologic malignancies: case report and review of the literature. Cancer 2001;92(9):2237-46.
- Elliott DC. An evaluation of the end points of resuscitation. J Am Coll Surg 1998;187(5):536-47.
- Tisherman SA, Barie P, Bokhari F, et al. Clinical practice guideline: endpoints of resuscitation. J Trauma 2004;57(4):898-912.
- Middleton P, Kelly AM, Brown J, Robertson M. Agreement between arterial and central venous values for pH, bicarbonate, base excess, and lactate. Emerg Med J 2006;23(8):622-4.
- Gallagher EJ, RodrÃguez K, Touger M. Agreement between peripheral venous and arterial lactate levels. Ann Emerg Med 1997;29(4):479-83.
- Forsythe SM, Schmidt GA. Sodium bicarbonate for the treatment of lactic acidosis. Chest 2000;117(1):260-7.
- Shapiro JI. Functional and metabolic responses of isolated hearts to acidosis: effects of sodium bicarbonate and Carbicarb. Am J Physiol 1990;258(6 Pt 2):H1835-9.
- Cooper DJ, Herbertson MJ, Werner HA, Walley KR. Bicarbonate does not increase left ventricular contractility during L-lactic acidemia in pigs. Am Rev Respir Dis 1993;148(2):317-22.
- Cooper DJ, Walley KR, Wiggs BR, Russell JA. Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled clinical study. Ann Intern Med 1990;112(7):492-8.
- Mathieu D, Nevière R, Billard V, Fleyfel M, Wattel F. Effects of bicarbonate therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis: a prospective, controlled clinical study. Crit Care Med 1991;19(11):1352-6.
- Adrogué HJ, Madias NE. Management of life-threatening acid-base disorders. First of two parts. N Engl J Med 1998;338(1):26-34.


