Contributed by Authors: Justin R Ng, Vinod Aiyappan, Zulfi Haneef, Nick A Antic, Affiliation: Adelaide Institute for Sleep Health, Repatriation General Hospital, Daw Park, SA 5000, Australia. Flinders University, Bedford Park, SA. Department of Neurology, Baylor College of Medicine, Houston, TX, USA Corresponding Author: Justin Raymond Ng, Adelaide Institute for Sleep Health, Repatriation General Hospital
In Brief
An abnormal electroencephalogram (EEG) pattern was noticed during an in-laboratory diagnostic polysomnogram, which was performed on a patient with symptoms of daytime fatigue and unrefreshing sleep. The clinical relevance of the EEG abnormality was considered in the context of the other information revealed in the patient’s medical history.
Case Vignette
A 61-year-old woman was referred for evaluation of daytime fatigue and unrefreshing sleep. Her Epworth Sleepiness Scale (ESS) was 6/24 and body mass index (BMI) was 38. Her medical history was significant for chronic low back pain, L3/L4 spinal canal stenosis and adjustment disorder with depressed mood. There was no history of epilepsy. Her medications included morphine sulphate controlled release 120 mg twice daily, gabapentin 600 mg twice daily (for pain control) and celecoxib 200 mg daily. The patient underwent a diagnostic laboratory sleep study. She consumed no caffeinated beverages on the day prior to the overnight study. Two thirty second consecutive epochs of her polysomnography (PSG) are shown in Figure 1 and 2.
Question:
What are the abnormalities seen in the polysomnogram (Figure 1 and 2)?
Figure 1: Representative recording of one 30-second epoch from the diagnostic polysomnography
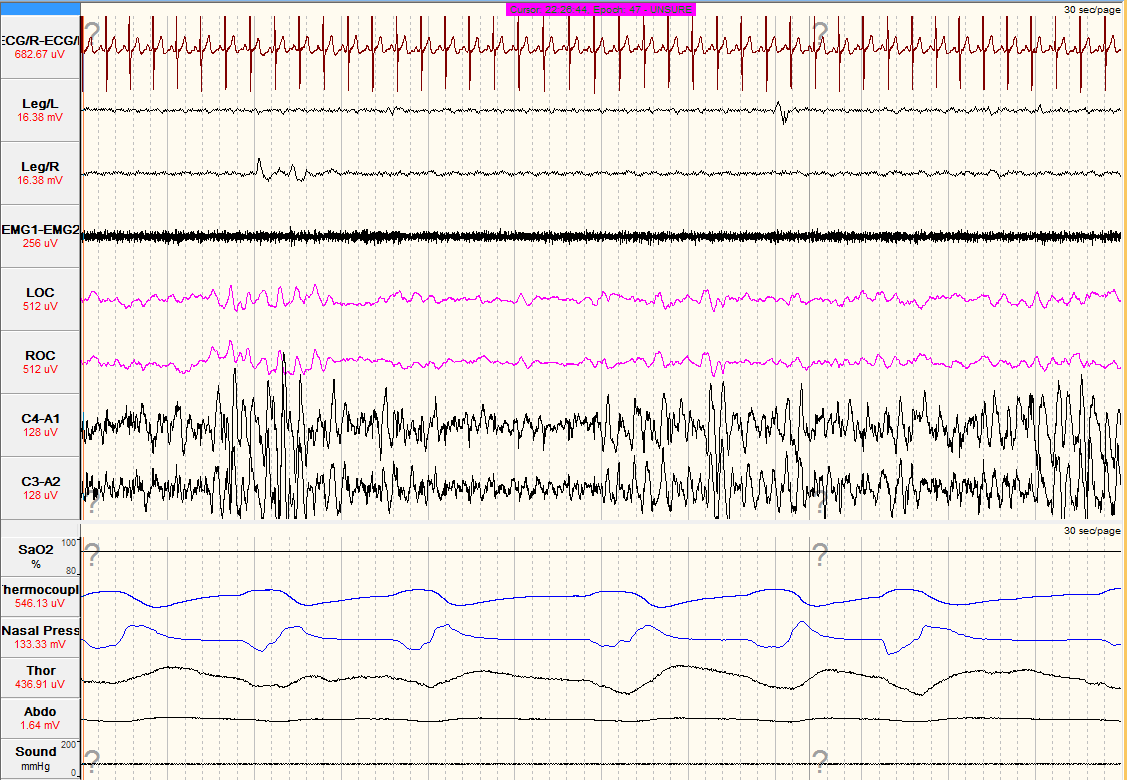
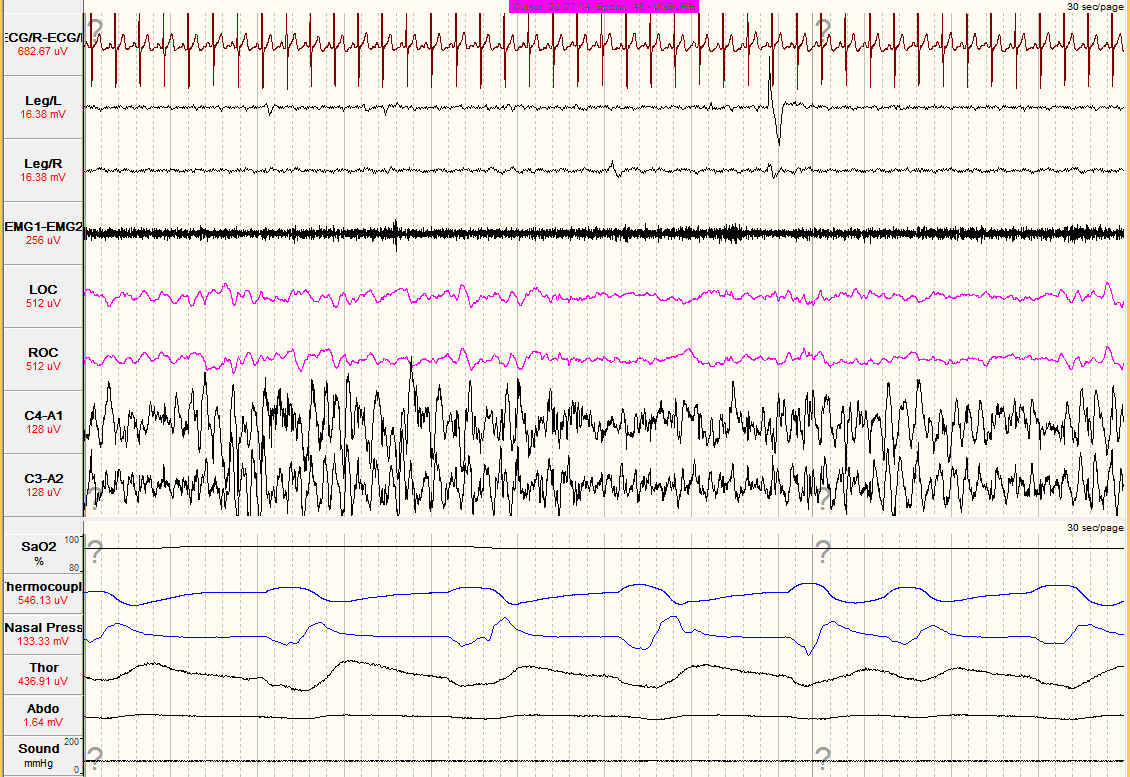
Figure 2: Representative recording of one 30-second epoch from the diagnostic polysomnography
Answer:
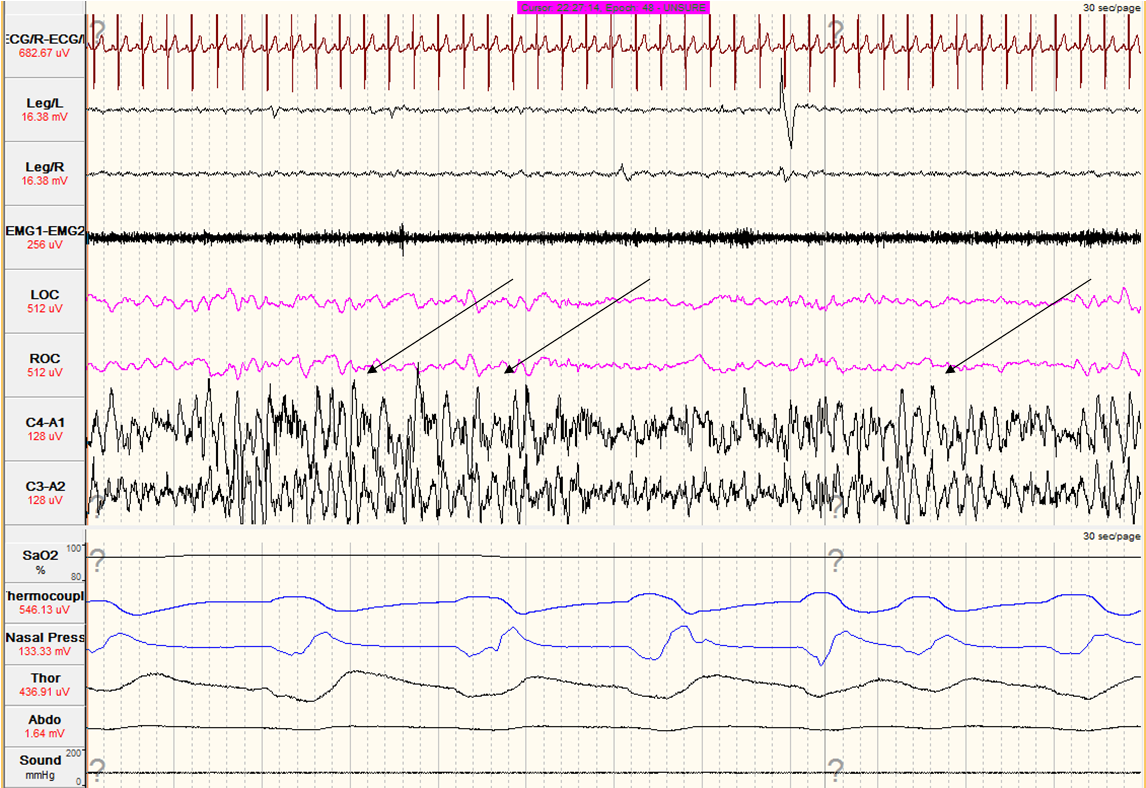
The diagnostic PSG shows an abnormal EEG pattern in C4-A1 and C3-A2 leads during sleep. The pattern consists of high amplitude, rhythmic, sharp contoured, non-evolving 3 to 4 Hz theta rhythm. This is suggestive of Subclinical Rhythmic Electrographic Discharge of Adults (SREDA) as shown in Figure 3 and 4 (arrows).
Figure 3: An example of Subclinical Rhythmic Electrographic Discharge of Adults as shown by the arrows
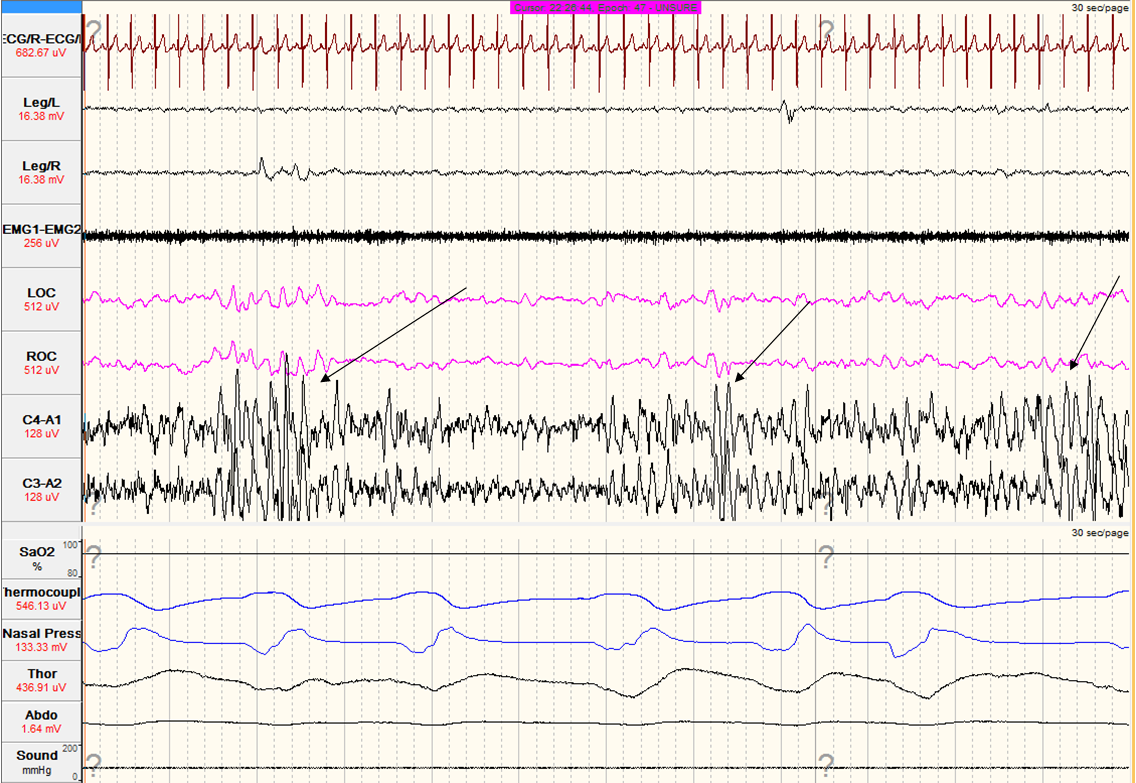
Figure 4: An example of Subclinical Rhythmic Electrographic Discharge of Adults as shown by the arrows
Discussion:
Subclinical rhythmic electrographic discharge of adults (SREDA) is an EEG pattern of uncertain significance1. This rare, but distinctive, rhythmic EEG pattern was first described by Westmoreland and Klass in 1981. They defined SREDA as “an unusual transient EEG pattern consisting of repetitive bilateral sharp contoured waveforms in the range of theta to delta frequency lasting for a few seconds to minutes, distributed mainly over the parietal and temporal regions, without subsequent evolution in frequency, distribution or morphology”2. There is an abrupt onset with a gradual offset and no postictal slowing of their EEG. It has a tendency to occur several times during a single EEG recording and is frequently present on subsequent recordings3. SREDA can evolve from an initial delta to a theta rhythm, making differentiation from seizures difficult.
SREDA tends to occur in wakefulness, often during hyperventilation and drowsiness. It occasionally occurs in sleep, both in the non rapid eye movement (NREM) and rapid eye movement (REM) stages2-3,4-6. During sleep, SREDA may be mixed with other normal physiological sleep figures such as sleep spindles3. Other supportive features on PSG of SREDA include the absence of changes in heart rhythm and the lack of ocular and muscular artefacts in the electrooculography (EOG) and electromyography (EMG) channels respectively3. In this case, SREDA was identified during NREM sleep with a typical pattern as described above. There were no changes in ECG, EMG or EOG channels.
SREDA is not associated with seizure activity before, during or after the episode. It is primarily seen in adults over the age of 601. The clinical significance of SREDA is uncertain but is likely to be benign with little or no clinical consequences7-8. Several observations by Naquet et al9 had suggested that transient hypoxia, ischaemia, cerebrovascular disease or a combination might have a role in the precipitation of SREDA. In this case, the oxygen saturation was stable at 93% on room air during the epochs with SREDA. There are many features of SREDA that still remain unexplained including the neurophysiological mechanisms underlying this activity and why it is more common in the elderly.
A limitation in the interpretation of this EEG is the reduced number of EEG channels recorded. Standard PSG recordings have only two channels of EEG limiting interpretation of certain findings such as SREDA. In particular, a similar appearance can also be seen in cyclic alternating pattern, which remains in the differential. The lack of parieto-temporal channels in the EEG makes this distinction challenging, as SREDA is more prominent in this location. However, the EEGs did not demonstrate the typical CAP cycles. Although challenging, it is important to recognise potential SREDA using limited EEG channels as the majority of standard PSGs will only have limited EEG channels available.
SREDA resembles epileptiform activity and can be misinterpreted as a true epileptiform pattern. Misinterpretation can result in unnecessary further investigations or the misdiagnosis of seizures with subsequent commencement of potentially harmful medications. A repeat diagnostic PSG study with a 16 channel EEG recording should be performed if there are clinical concerns about the EEG abnormality recorded.
Follow up:
Apart from showing SREDA pattern, the sleep study showed uncomplicated snoring with no evidence of significant sleep disordered breathing or hypoxia. The patient’s symptoms of daytime fatigue were thought to be due to a combination of her medications, underlying depression and obesity. Overall, the distinctive EEG features, lack of overt clinical signs and absence of other supportive PSG features suggested a nonepileptic phenomenon. No further investigations for the SREDA were required.
References:
- Dash GK, Radhakrishnan A. What does “subclinical rhythmic electrographic discharge of adults” in EEG signify? Journal of Clinical Neurophysiology. 2013; 30(3):255-60.
- Westmoreland BF, Klass DW. A distinctive rhythmic EEG discharge of adults. Electroenceph Clin Neurophysiol 1981; 51:186-191
- Brigo F, Ausserer H, Nardone R et al. Subclinical rhythmic electroencephalogram discharge of adults occurring during sleep: A diagnostic challenge. Clin EEG Neurosci 2013; 44(3):227-231
- Wennberg R. Atypical SREDA in sleep. Electroenceph Clin Neurophysiol. 2013;124(2):425-6.
- Westmoreland BF. Benign Electroencephalographic Variants and Patterns of Uncertain Clinical Significance. In: Ebersole JS, Pedley TA , editors. Current Practice of Clinical Electroencephalography, 3rd ed. Lippincott Williams & Wilkins, 2003. p. 235-245.
- Fleming WE, Avidan A, Malow BA. Subclinical rhythmic electrographic discharge of adults (SREDA) in REM sleep. Sleep Med 2004;5(1):77-81.
- Westmoreland BF, Klass DW. Unusual variants of subclinical rhythmic electrographic discharge of adults (SREDA). Electroenceph Clin Neurophysiol 1997; 102(1):1-4.
- Begum T, Ikeda A, Takahashi J, Tomimoto H, Shimohama S, Satow T, Nagamine T, Fukuyama H, Shibasaki H. Clinical outcome of patients with SREDA (subclinical rhythmic EEG discharge of adults). Intern Med 2006; 45:141-144.
- Naquet R, Franck G, Vigouroux R. New data on some paroxysmal discharges in the parieto-temporo-occipital pathways noted in man. Zentralbl.


