A 65-year-old man presents from his primary physician’s office out of concern for possible obstructive sleep apnea. He describes relatively good sleep quality, but endorses loud, disruptive snoring and witnessed apneas. Physical exam is significant for oropharyngeal crowding and obesity. A home sleep apnea test is initially ordered. On the way out of the room, the patient notes offhandedly that he also fights in his sleep, and that he frequently acts out his dreams. His wife, who has accompanied him to this appointment, agrees with the patient, saying that he mutters a lot, and on a couple of occasions he has hit her hard enough to leave bruises. The home sleep apnea test is cancelled and a diagnostic polysomnogram is ordered instead.
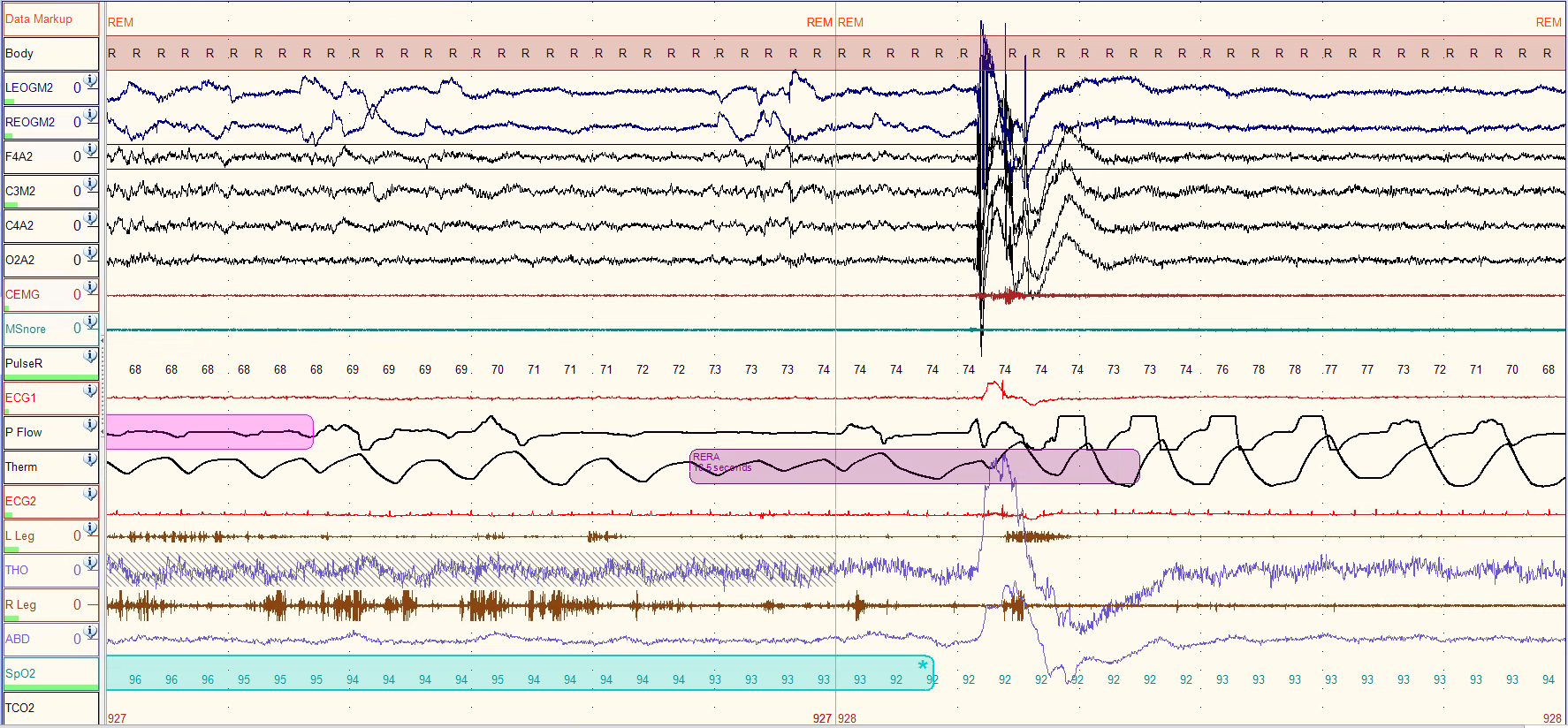
A representative 1-minute epoch of REM sleep is shown below. The light pink segment toward the left is the end of a hypopnea, and the purple segment near the middle is a respiratory effort-related arousal (RERA). (Click image for larger version.)
The patient’s polysomnogram was fairly normal except for moderate obstructive sleep apnea (apnea-hypopnea index [AHI] of 29.5 events/hr), and REM sleep without atonia (RWA).
REM behavior disorder can be diagnosed in the correct clinical context (fighting in sleep or acting out dreams, very commonly), with the appearance of RWA. However, sometimes RWA can occur in the setting of sleep disordered breathing, and it may be difficult to establish whether the observed movements result from respiratory events.
As such, the patient underwent another polysomnogram while being treated with autotitrating PAP (pressure range 6-14 cm H2O). This study showed normal sleep architecture and an AHI of 1.3 events/hr. However, the patient still had RWA. As such, a presumptive diagnosis of REM behavior disorder was made. The patient was started on melatonin with good symptomatic effect and was referred to a neurologist since most patients diagnosed with REM behavior disorder will ultimately develop an alpha synucleopathy (Parkinson’s disease, Lewy body dementia, or multiple systems atrophy).


