Article:
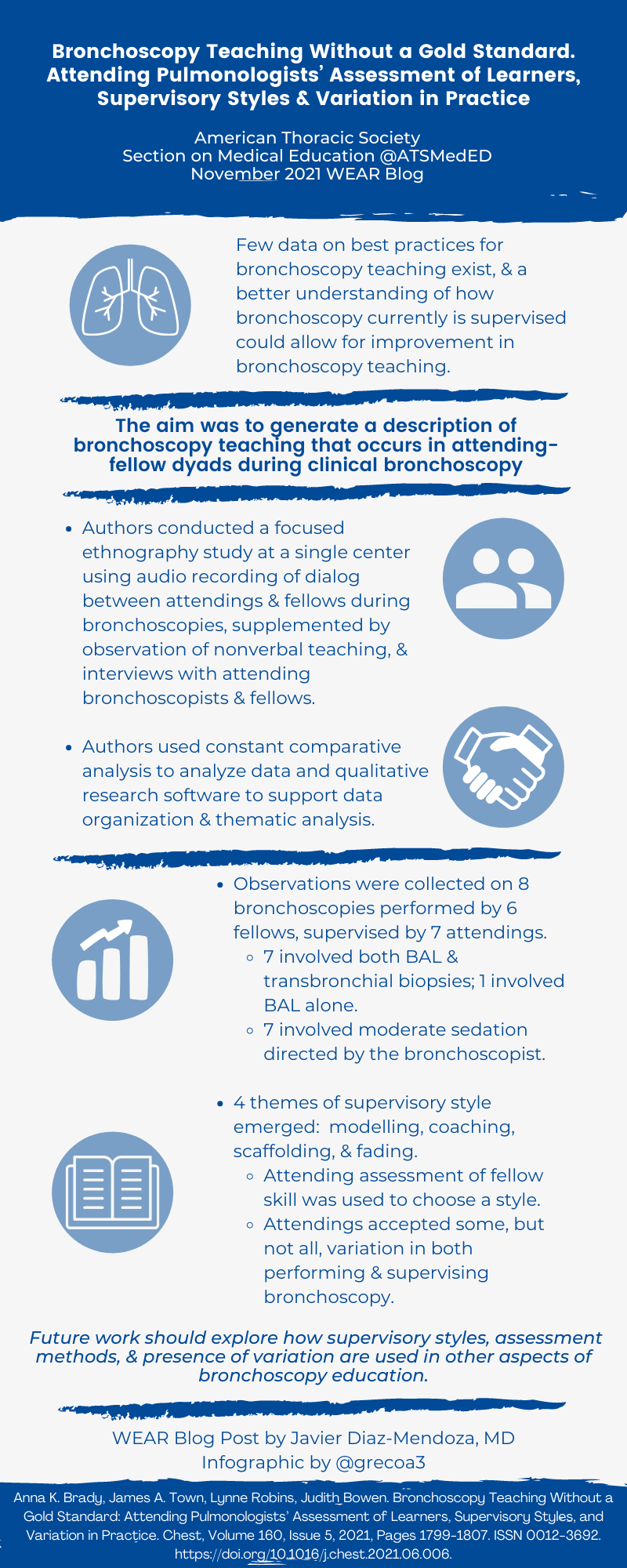
Bronchoscopy Teaching Without a Gold Standard. Attending Pulmonologists' Assessment of Learners, Supervisory Styles and Variation in Practice
Anna K. Braddy, MD; James A. Town, MD; Lynne Robins, PhD; and Judith Bowen, MD, PhD
Summary:
There is little data about best practices for bronchoscopy teaching and how to balance fellow autonomy with patient safety. The aim was to learn, define and characterize how attendings supervise bronchoscopic procedures and how they manage this balance. The authors used an ethnographic approach, direct observation with data collection (audio recordings, field notes and semi structured interviews) from the interaction between attendings and fellows during eight bronchoscopic procedures done in a single center between 2016 and 2017. The teaching styles used by the attendings were found to follow the "cognitive apprenticeship" pattern previously described (modeling, coaching, scaffolding and fading). They were chosen based on the level of expertise shown by the fellow. Techniques used to assess expertise level of fellows were variable (fellow's time in the program, questions, observation and handoffs). Sometimes alternating teaching styles were seen within the same bronchoscopic procedure based on the level of difficulty. Many attendings accepted variation of fellows' techniques except for selective parts of the procedure where patient safety or better educational experience was thought could be uncertain. The interpretation of the study: attendings evaluate fellows' level of expertise before choosing a teaching style; and variation of fellows' technique is selectively accepted by attendings.
Interview:
JDM: One of the topics discussed in the article was about giving autonomy to fellows based on an assessment. When working with a fellow for the first time, what is the ideal way to assess their skill set prior to starting the procedure?
JT: I think "pre-gaming" with the fellow beforehand is vitally important. Specifically, discussing the case and plan and using some specific probing questions tailored to the fellow's anticipated experience level. I use it to build the learning climate to feel relatively "low stakes" and relaxed and I try not to guide the fellow too much unless they are way off base. More bluntly, the number of procedures they have done and asking for their self-reflection on prior bronchoscopies also helps me anticipate their skill level and plan what we're going to focus on together. For example, a fellow doing their first few bronchoscopies may only be able to discuss the indications for the procedure and interpret the imaging but struggle to describe (or visualize) the anatomy and technical aspects of the procedure. On the other hand, a senior fellow may only need coaching to "think out loud" and identify specific areas for feedback.
Despite the pre-procedural assessment, I think the supervising faculty also has to adapt as the procedure unfolds; there is always the potential for an unknown and our ultimate goals are patient safety, learner safety and a successful procedure. I learn a lot by how the fellow communicates with the patient and staff, sets up the room, approaches sedation, responds to questions or tips, etc. Some of those unheralded microskills, like providing topical anesthesia, can make or break a procedure so if they struggle with that I shift to a more modeling or coaching approach until I feel confident they can take over again.
JDM: Accepting variation of a trainee's bronchoscopic techniques could be difficult for a junior faculty, who may still have limited teaching experience. What advice would you provide them when teaching bronchoscopy?
JT: We all continue to learn long after formal training ends, so acknowledging that perpetual growth is important to ease the tension for both the learner and faculty. Even if the faculty has limited experience, it almost certainly dwarfs the fellow's so you could focus on excellent execution of the bread & butter steps of the process. Early on, just pick one or two things for the fellow to work on and don't try to teach too much. The primary goal of the encounter should be "How do we do this procedure together safely and learn the most from it?". Teach about how you would do it, talk out loud, explain your reasoning (including recognizing where there is uncertainty or alternative "styles"). It's not each faculty member's job to teach variation and all that there is to know about bronchoscopies, but we should acknowledge that there are many ways to get the job done. As a junior faculty member, I am learning everyday so I also look at these encounters as training experiences on how to teach better.
JDM: Based on the learner's level of expertise, 4 teaching styles were presented in this article (modeling, coaching, scaffolding and fading). What is your opinion about standardization of teaching styles among the faculty within an institution when it comes to bronchoscopy? And how could that impact bronchoscopy competency in fellows?
JT: I think it's worthwhile for an institution and each faculty member to be able to vary the learning experience – different learners and situations merit different approaches. An inexperienced, nervous fellow or a higher risk situation will need more guidance or more attention to the safety of the procedure while maintaining a good educational climate for the learner to be successful down the road. Conversely, a senior fellow may benefit more from simulating life outside of the training institution - i.e. a very "fading" approach so the learner is challenged to flex their autonomy as much as is feasible.
As an institution, you want trainees to leave as competent as possible and be able to navigate their way through unpredictable situations in the future as well as pass their knowledge on to others. If trainees have a rigid conception of the "right way" to do something and their next institution has a different culture or style, it could pose challenges working with staff, maintaining confidence in their professional identity and training and slow their progression. Ultimately, competence is defined by doing the right thing regardless of the situation, so I think training needs to prepare graduates to be adaptable.
JDM: And lastly, what would you consider to be the ideal faculty-fellow interaction while teaching bronchoscopy?
JT: It should be a partnership between the fellow and faculty with the primary goals being safety (for the patient and the learner) and creating an optimal learning climate. Both the faculty and the fellow need to collaborate to tailor the experience to the dyadic interaction by targeting the learning towards the fellow's needs while leveraging the strengths of the faculty. I think it's important for the faculty to model ideal procedural and learning behaviors, including seeking and giving specific feedback and engaging in self-reflection about how the experience went. Establishing trust and rapport builds that relationship and creates a safer space for learners to grow and excel. In my opinion it also makes for a more rewarding experience for everyone. Lastly, it's important to be able to give critical feedback and intervene when things are unsafe, which is easier to do if your goals as a learner-teacher pair are aligned and you've created a safe learning climate.
Blog post author
Dr. Javier Diaz-Mendoza, MD, is an Associate Professor of Medicine in the Division of Pulmonary and Critical Care at Henry Ford Hospital-Wayne State University. He serves as Program Director of the Interventional Pulmonology fellowship and Director of Bronchoscopy Education for the Pulmonary and Critical Care Fellowship. His educational interests include curriculum development for achievement of procedural competencies and use of assessment tools for advanced bronchoscopic procedures.
Article author

Dr. James Town, MD, is an Assistant Professor in the Division of Pulmonary, Critical Care and Sleep at the University of Washington. He serves as Director of the Medical Intensive Care Unit at Harborview Medical Center. His professional interests include medical education, quality improvement and interprofessional collaboration.


