Kevin L Kovitz, MD, MBA
Professor of Medicine and Surgery, University of Illinois at
Chicago and Director, Chicago Chest Center
No Conflicts.
National coverage for lung cancer screening has arrived. In February 2015, Centers for Medicare & Medicaid Services (CMS) issued a final coverage policy. Heretofore, screening programs have had varying levels of success in attracting providers and patients alike with the major barrier being lack of reimbursement. The purpose of this discussion is separate from the utility of screening. Rather, the focus is on obtaining coverage for the patient encounters and scans required. The Affordable Care Act and the CMS lung cancer screening policy significantly change coverage.
There are 2 main areas to understand, CMS coverage and commercial carrier coverage.
CMS Coverage
From a CMS perspective, we can take the specific criteria from their announcement.1 The ATS, like many organizations, submitted comments to improve and clarify the initial CMS proposal. Specifically, the ATS recommended extending the screening coverage to include Medicare beneficiaries aged 75-80, sought clarification on the shared decision making visits, recommended clarifying language on the term “asymptomatic” and noted the importance of a multidisciplinary team in diagnosing and managing lung cancer. The final CMS policy addresses these issues, with the age reaching 77, shared decision making clarified, and “asymptomatic” focused to symptoms related to lung cancer. Practitioners and programs should carefully review the final policy prior to establishing a site-specific screening protocol.
The CMS proposal is very detailed, mostly follows the National Lung Screening Trial (NLST) criteria, and requires specific personnel, shared decision making with the patient, specific documentation, smoking cessation counseling, detailed orders, specific radiology requirements, and participation in a registry. The specific CMS decision summary of the policy, copied directly from the website, is noted below1 for reference as there are extensive and very detailed requirements. Please review these carefully.
Private Insurance
Commercial carriers face a different issue. As most are aware, the USPSTF has recommended lung cancer screening for a broader age range.2 The grade of B was given for the validity of the supporting data. According to the Affordable Care Act, 3 all preventative services that received an A or B grade from the USPSTF must be covered by private insurance at no costs to the consumer.3 Commercial carriers are required incorporate category A and B recommendations with the plans annual renewal. It is important to note that the annual renewal date for private plans can happen through the calendar year. Private insurance coverage for lung cancers screening did not necessarily start in January for private patients. Providers should consult with patients and insurance companies to ensure lung cancer screening is covered.
Age and Coverage Policy
The coverage criteria are similar in all respects aside from age. This is not an issue in most situations as the 55-64 year old and the 65-77 year old with commercial insurance or Medicare should be covered. The most common scenario is of the younger patient with commercial insurance and the older group with Medicare. Interestingly, the 78-80 year old with Medicare is not covered unless they have commercial insurance as primary coverage. The commercially insured older patient is likely to represent a small group and CMS coverage is an issue if one is of the opinion that screening needs to be done in this age group.
Coding
Coding is multifactorial. However, there is no specific CPT code for the Evaluation and Management of a patient that presents for Lung Cancer Screening evaluation. Traditional outpatient consults (where applicable), new patient or established patient E & M coding should be used. The E & M selected must be commensurate with the level of service as determined by specific actions or counseling as one would with any visit. The diagnoses may include, but are not limited to: special screening for malignant neoplasm of the respiratory organs, V76.0 (ICD-9) or Z12.2 (ICD-10)4 and all diagnoses appropriate to the patient’s problems. Consider including a code for the tobacco history such as nicotine dependence (ICD-9 305.1, ICD-10 F17.200) or history of same (ICD-9 V15.82, ICD-10 Z87.891). The tobacco code is not specified but makes sense as these patients need a smoking history and pack years need to be documented in order to qualify for screening.
The radiologist will have a specific HCPCS code of S8032 Low-dose computed tomography for lung cancer screening.5 The above summary reflects the current point in time. Practitioners and programs are urged to carefully review the final policy before establishing program policies. Additionally, it is important to review the policies of individual commercial carriers as they often differ from CMS.
References
- http://www.cms.gov/medicare-coverage-database/details/ nca-decision-memo.aspx?NCAId=274 accessed 2/10/15). See below.
- Moyer VA on behalf of the U.S. Preventive Services Task Force. Screening for lung cancer: U.S. preventive services task force recommendation statement. Ann Intern Med. 2014;160(5):330-338.
- http://www.law.cornell.edu/cfr/text/29/2590.715-2713 (accessed 12/3/14) by way of http://newsatjama.jama.com/2014/10/15/jama-forum-lung-cancer-screening-andevidence-based-policy/ accessed 12/3/14.
- Current Procedural Terminology (versions 9 and 10) and Healthcare Procedural Coding System (HCPCS) codes referenced are the property of the American Medical Association.
The following is copied directly from the CMS website1: *The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to add a lung cancer screening counseling and shared decision making visit, and for appropriate beneficiaries, annual screening for lung cancer with low dose computed tomography (LDCT), as an additional preventive service benefit under the Medicare program only if all of the following criteria are met:
Beneficiary eligibility criteria:
- Age 55 – 77 years;
- Asymptomatic (no signs or symptoms of lung cancer);
- Tobacco smoking history of at least 30 pack-years (one pack-year = smoking one pack per day for one year; 1 pack = 20 cigarettes);
- Current smoker or one who has quit smoking within the last 15 years; and
- Receives a written order for LDCT lung cancer screening that meets the following criteria:
- For the initial LDCT lung cancer screening service: a beneficiary must receive a written order for LDCT lung cancer screening during a lung cancer screening counseling and shared decision making visit, furnished by a physician (as defined in Section 1861(r)(1) of the Social Security Act) or qualified non-physician practitioner (meaning a physician assistant, nurse practitioner, or clinical nurse specialist as defined in §1861(aa)(5) of the Social Security Act). A lung cancer screening counseling and shared decision making visit includes the following elements (and is appropriately documented in the beneficiary’s medical records):
- Determination of beneficiary eligibility including age, absence of signs or symptoms of lung cancer, a specific calculation of cigarette smoking pack-years; and if a former smoker, the number of years since quitting;
- Shared decision making, including the use of one or more decision aids, to include benefits and harms of screening, follow-up diagnostic testing, over-diagnosis, false positive rate, and total radiation exposure;
- Counseling on the importance of adherence to annual lung cancer LDCT screening, impact of comorbidities and ability or willingness to undergo diagnosis and treatment;
- Counseling on the importance of maintaining cigarette smoking abstinence if former smoker; or the importance of smoking cessation if current smoker and, if appropriate, furnishing of information about tobacco cessation interventions; and
- If appropriate, the furnishing of a written order for lung cancer screening with LDCT.
- For subsequent LDCT lung cancer screenings: the beneficiary must receive a written order for LDCT lung cancer screening, which may be furnished during any appropriate visit with a physician (as defined in Section 1861(r)(1) of the Social Security Act) or qualified nonphysician practitioner (meaning a physician assistant, nurse practitioner, or clinical nurse specialist as defined in Section 1861(aa)(5) of the Social Security Act). If a physician or qualified non-physician practitioner elects to provide a lung cancer screening counseling and shared decision making visit for subsequent lung cancer screenings with LDCT, the visit must meet the criteria described above for a counseling and shared decision making visit.
- Written orders for both initial and subsequent LDCT lung cancer screenings must contain the following information, which must also be appropriately documented in the beneficiary’s medical records:
- Beneficiary date of birth;
- Actual pack - year smoking history (number);
- Current smoking status, and for former smokers, the number of years since quitting smoking;
- Statement that the beneficiary is asymptomatic (no signs or symptoms of lung cancer); and
- National Provider Identifier (NPI) of the ordering practitioner.
Reading radiologist eligibility criteria:
- Board certification or board eligibility with the American Board of Radiology or equivalent organization;
- Documented training in diagnostic radiology and radiation safety;
- Involvement in the supervision and interpretation of at least 300 chest computed tomography acquisitions in the past 3 years;
- Documented participation in continuing medical education in accordance with current American College of Radiology standards; and
- Furnish lung cancer screening with LDCT in a radiology imaging facility that meets the radiology imaging facility eligibility criteria below.
Radiology imaging facility eligibility criteria:
- Performs LDCT with volumetric CT dose index (CTDIvol) of ≤ 3.0 mGy (milligray) for standard size patients (defined to be 5’ 7” and approximately 155 pounds) with appropriate reductions in CTDIvol for smaller patients and appropriate increases in CTDIvol for larger patients;
- Utilizes a standardized lung nodule identification, classification and reporting system;
- Makes available smoking cessation interventions for current smokers; and
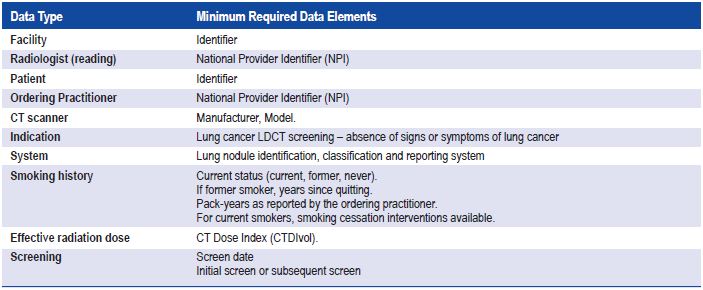
- Collects and submits data to a CMS-approved registry for each LDCT lung cancer screening performed. The data collected and submitted to a CMS-approved registry must include, at minimum, all of the following elements: