Although CMS issued the final payment rules for both the Medicare Physician Fee Schedule (MPFS) and the Medicare Hospital Outpatient Prospective Payment System (HOPPS) in November of 2015, the payment calculations for both rules had many errors. The following two tables provide corrected information for both physician office payments and hospital outpatient payments.
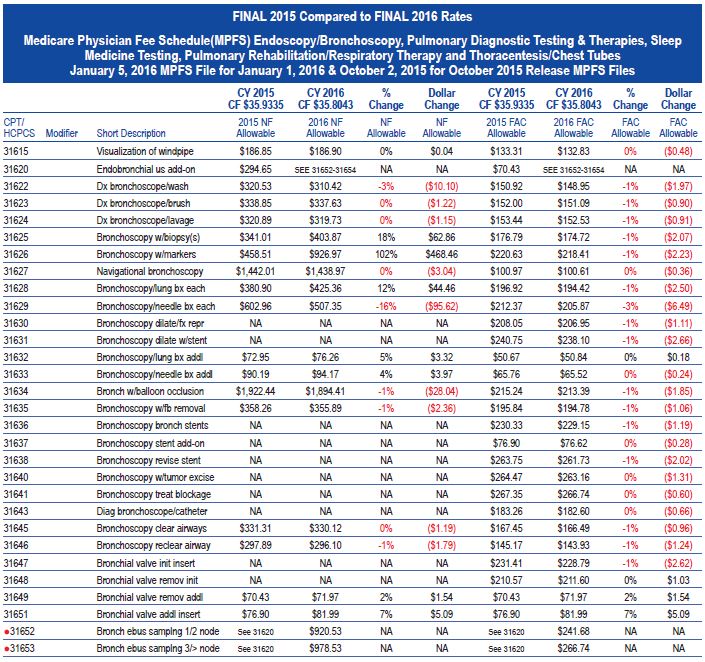
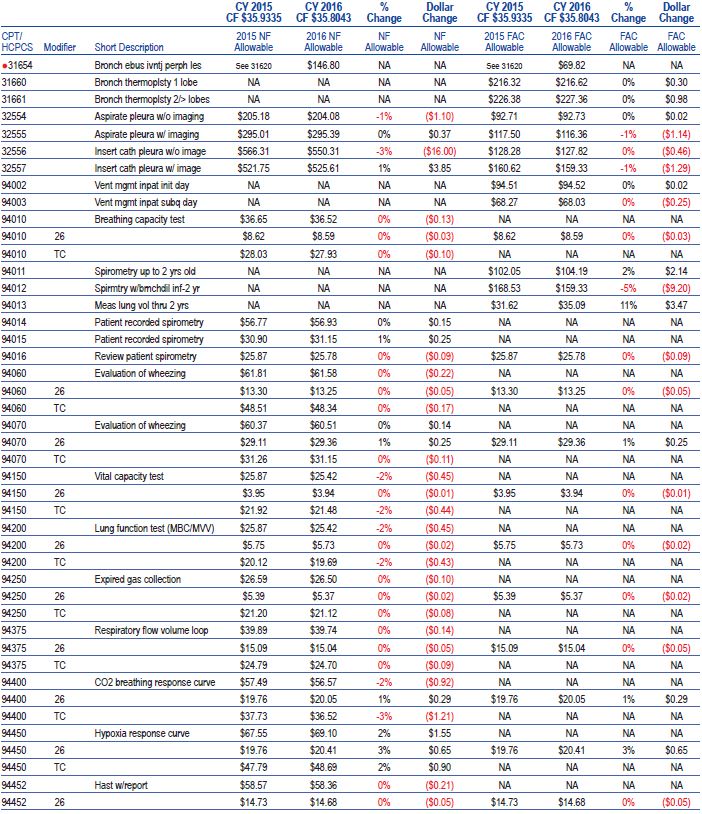
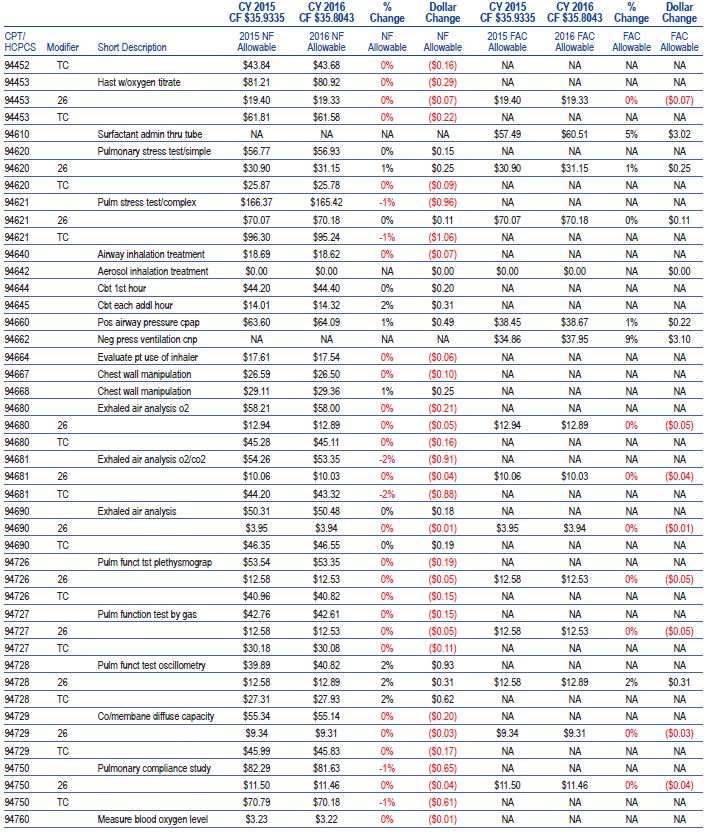
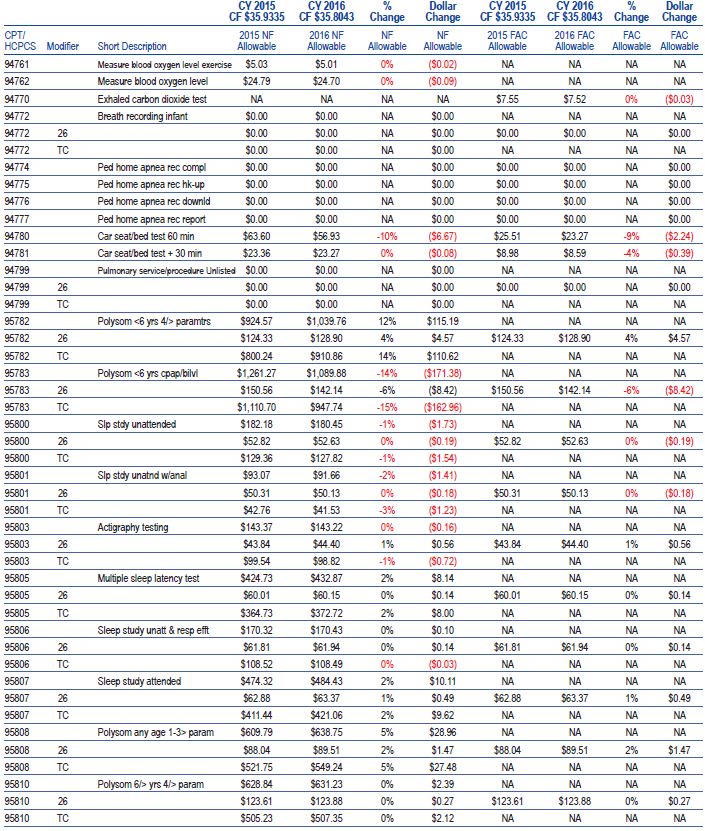
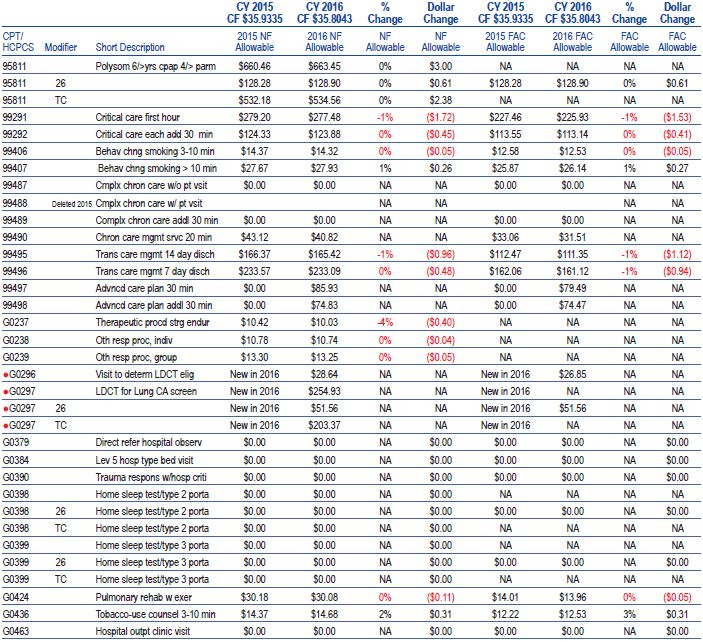
Medicare Physician Fee Schedule
Payments for pulmonary, critical care and sleep medicine saw only minor variation in the MPFS rule for 2016. Most of the payment changes were driven by system wide trends, such as across the board practice expense payment cuts, rather than factors specific to the individual service.
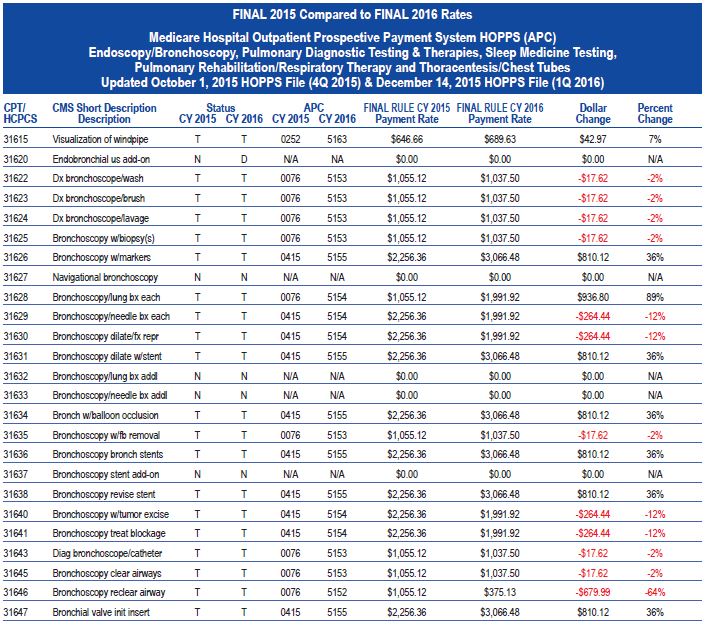
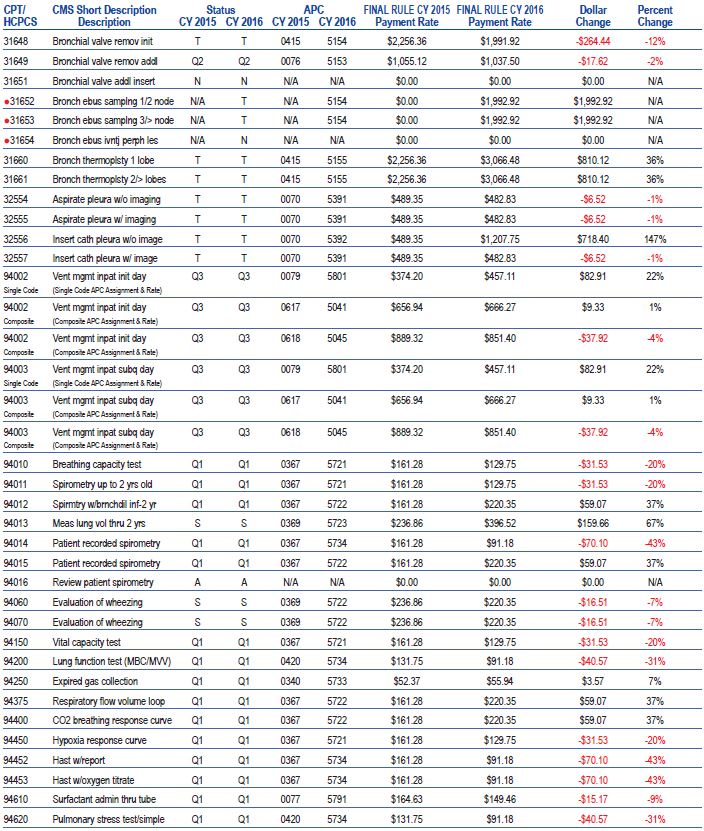
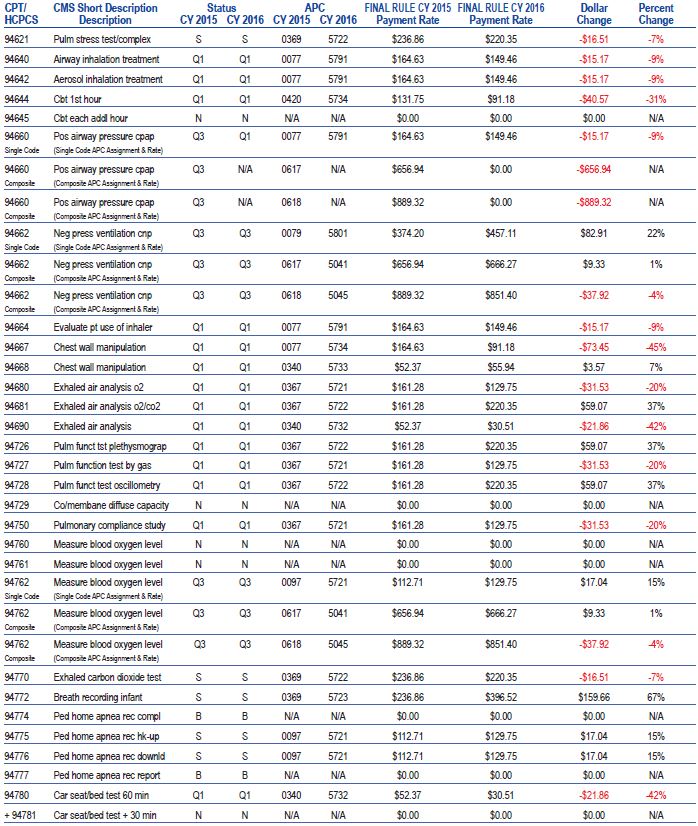
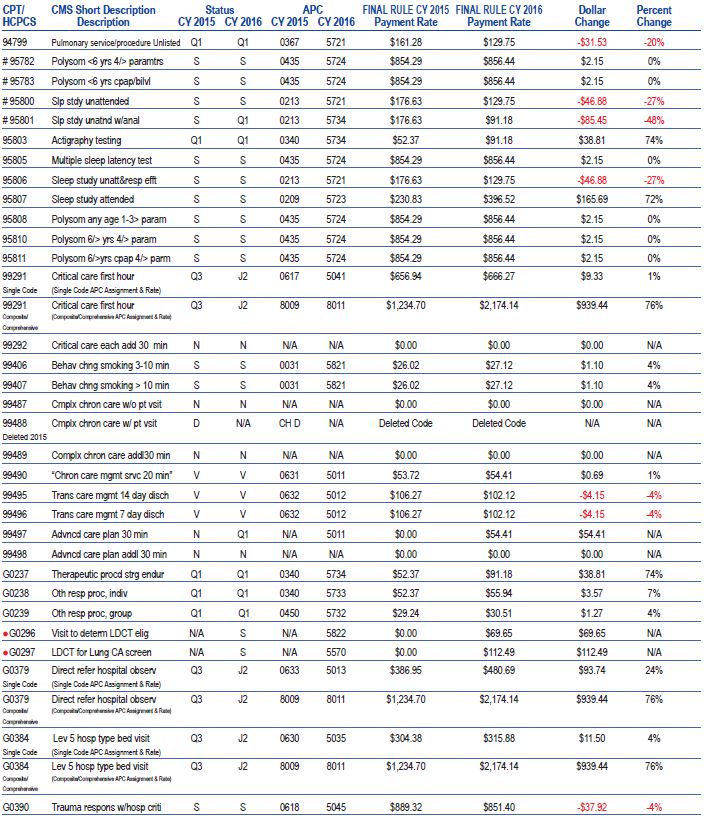
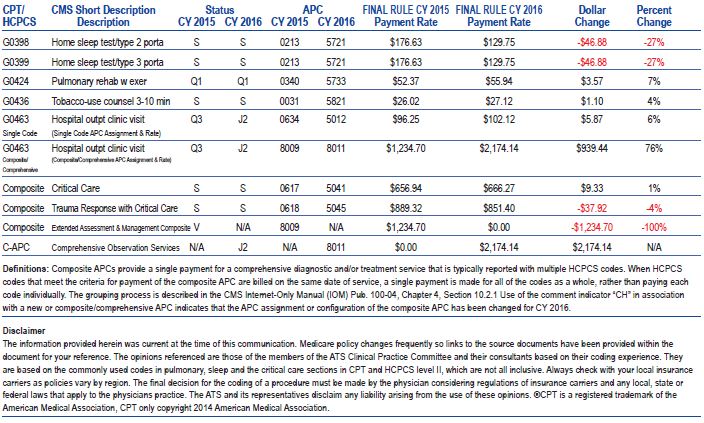
Hospital Outpatient Prospective Payment System
HOPPS 2016 payments for pulmonary, critical care and sleep service saw significant variation from 2015 payment levels. The majority of the payment variation was driven by consolidation of Medicare Ambulatory Payment Classifications (APC) levels for outpatient services. The APC consolidation effort creates “winners” (example: 31626 – Bronchoscopy w/placement of markers +36%) and “losers” (example: 31646- bronchoscopy, subsequent therapeutic aspiration of airways -64%) across many areas of pulmonary service including pulmonary function tests, bronchoscopic procedures, ventilator management and sleep testing. The consolidation of APCs in the pulmonary community is a continuation of CMS’s efforts to decrease the number of APC levels across all physician specialties.
Reimbursement for pulmonary rehabilitation (G0424 – pulmonary rehabilitation respiratory +7%) and respiratory therapy (G0237 - Therapeutic procedure to increase strength or endurance of respiratory muscles, face to face, one on one, 15 minutes each - +74%) payments are both increased in 2016.