
This summer, CMS issued the proposed 2016 rule for the Hospital Outpatient Prospective Payment System. The rule touched on a number of areas of interest to ATS members. Below is a quick summary of key issues:
Pulmonary Rehabilitation and Respiratory Therapy Codes
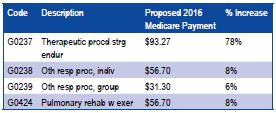
On the plus side, CMS is proposing to increase the payment for pulmonary rehabilitation (G0424) and respiratory therapy codes (G0237, G0238, G0239) provided in hospital outpatient departments for 2016.
APC Consolidation
CMS is proposing to consolidate the Ambulatory Payment Classification (APC) across a broad range of outpatient hospital services, including services that impact interventional bronchoscopy procedures, pulmonary function tests and sleep testing. The proposed APC consolidation will likely create payment “winners and losers” in each of the impacted APC categories. However, the proposed rule initiates so many proposed policy changes it is difficult to estimate the magnitude of impact caused by APC consolidation. While estimating the exact impact is challenging, it appears the overall impact on payments for pulmonary and sleep services will be minimal.
Chronic Care Codes
In the proposed rule CMS issued a clarification on the appropriate use of chronic care codes (CPT 99490) but did not propose to allow providers to use complex chronic care codes (CPT 99487/99489).
Lung Cancer Screening Shared Decision Making Visit Code
Also in the proposed CMS Hospital Outpatient Prospective Payment rule is CMS’s proposal for coding the “shared decision making visit” needed for CT lung cancer screening. As you may recall, CMS issued coverage policy for CT lung cancer screening earlier this year. One of the requirements for lung cancer screening was a “shared decision making visit” for patients and providers to discuss the risks and benefits of lung cancer screening. However, in issuing the coverage policy, CMS did not outline how to code and bill for the shared decision making visit.
In the proposed rule, CMS has created new G codes for the shared decision making. Each visit is proposed by CMS to be approximately 15 minutes long with a work RVU of 0.52 therefore an approximate payment of $20.00. What is unclear in the CMS proposal is whether thecode can be used with an E&M service or whether CMS envisions the code as a stand-alone service only. The ATS believes the code should be available in both situations, as a stand-alone service or in combination with an E&M service.

