
In related news, CMS released the proposed 2016 Medicare Physician Fee Schedule rule that proposes payment rates and policies for physicians and other Part B providers for the coming year. The rule covers a number of areas of interest to the ATS including:
Potentially Mis-valued Services Under the Physician Fee Schedule
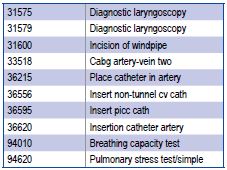
CMS has identified a number of CPT codes as “potentially mis-valued.” That means CMS is requesting/requiring the provider community to resurvey these codes to ensure they have the appropriate relative values within the overall coding system. The ATS is concerned that CMS’s selection is driven more by cost saving potential than actual selection of misvalued codes. If CMS moves forward with its plan to resurvey the identified codes, many codes of interest to ATS members will be affected, including:
Practice Expense, Malpractice Expense, and Physician Work Values
CMS has proposed to accept the practice expense values and malpractice values for a number of recently surveyed pulmonary codes. This is welcome news. However, CMS has rejected work values for the new endobronchial ultrasound codes. The ATS is concerned that CMS rejected the physician work values recommended by the ATS and the AMA RUC. ATS will provide comments to CMS supporting our recommended work values.
Elimination of Refinement Panels
In related news, CMS has proposed eliminating the “Refinement Panel”. These panels allow an appeal by the physician community with CMS for any code value lowered from the RUC recommendations. The refinement panels, while cumbersome, have been the physician communities’ only means of appealing CMS’s decisions on work values. The ATS strongly opposed CMS’s proposal to eliminate the refinement panels.
Advance Care Planning
The ATS strongly supports CMS’s proposal to pay for voluntary Advance Care Planning services (CPT 99497 and 99498). CMS finalized and later rescinded a similar policy in the 2011 final rule, bending to the political firestorm created by “death panel” demagoguery. While the ATS is disappointed it took CMS 4 years to move forward with this proposal, we are pleased that it has finally arrived. Allowing physicians and Medicare beneficiaries to voluntarily discuss and plan the care for life-threatening and end-of-life situations will improve care outcomes and reduce emotional stress on Medicare beneficiaries, their families and medical staff.
Quality Measures
The proposed rule also included small changes to a number of physician quality measures that touch on pulmonary diseases. Below is a quick summary of the proposed quality measures impacting pulmonary and critical care medicine;
NQF/PQRS 0028/226 –Preventive Care: Tobacco Use: Screening and Cessation Intervention
The ATS notes this measure has been included in several measures groups for 2016 and beyond including Cardiovascular Prevention Measures Group, Diabetes Retinopathy Measures Group, Diabetes Measures Group and the Preventive Care Measures Group.
Coordinating Care: Emergency Department Referrals:
CMS is proposing to measure emergency department efforts to contact the patient’s primary care physician in cases of asthma exacerbation and chest pain that do not result in an inpatient stay. While the ATS is generally supportive of quality measures to document and improve the effective coordination of care between the emergency room and primary care provider, we are concerned the proposed measure is not NQF endorsed (or endorsed by any other quality organization).
Post-Anesthetic Transfer of Care Measure: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU):
CMS is proposing to include the “checklist” measure for transfer of patients to intensive care units. . While we are generally supportive of quality measures to document and improve the effective transfer of care within a hospital, we are concerned the proposed measure is not NQF endorsed (or endorsed by any other quality organization). We are unaware of any studies that demonstrate quality improvements with the adoption of checklists for transfer of patients to the ICU.
Tuberculosis Prevention for Psoriasis, Psoriatic Arthritis and Rheumatoid Arthritis Patients on a Biological Immune Response Modifier:
CMS is proposing to adopt a TB prevention measure for patients on biological immune response modifiers.

