A 39-year-old Caucasian woman presents to the emergency department with a one-week history of fever and diffuse muscle aches. She also reports a one-day history of pain and swelling in her left inguinal area in addition to diffuse pain throughout her right thigh with overlying erythematous skin changes.
One week prior to presentation, she was seen by her primary care physician with complaints of fevers, chills, and diffuse muscle aches. She was noted to have marked pyuria on routine urinalysis, and was started on levofloxacin for suspected urinary tract infection. She subsequently developed painful swelling of her left forearm that was believed to be flouroquinolone-induced tendonitis and antibiotic therapy was switched from levofloxacin to ciprofloxacin with temporary resolution of her symptoms.
The patient was also seen by her gynecologist three days prior to presentation, with recurrence of her symptoms. A pelvic exam at that time was unremarkable. Cultures taken from the vaginal canal and a repeat urinalysis were both unremarkable. She was continued on ciprofloxacin and doxycycline was added for additional antimicrobial coverage. Despite the additional antibiotic, her symptoms worsened, with persistent fevers and myalgias in addition to generalized weakness and nausea.
Physical Exam
On physical exam the patient was found to be febrile with a temperature of 102 degrees Fahrenheit. Her heart rate was 80 with a blood pressure of 100/60. Her respiratory rate was 18 with an oxygen saturation of 100% on room air.
She appeared ill and uncomfortable. Although no cervical lymphadenopathy was appreciated, the musculature of her neck was noted to be diffusely tender to palpation. Her cardiovascular exam disclosed no murmurs and her pulmonary exam was unremarkable. Her abdomen was found to be diffusely tender to palpation without peritoneal signs or organomegaly. An enlarged tender lymph node was noted in her left inguinal region without surrounding erythema or fluctuance. The musculature of her extremities was found to be diffusely tender to palpation and a patchy, macular, blanching rash was noted over her trunk and extremities.
Lab
White blood cell count 13,400/mm3, Hemoglobin 11.4 g/dL, Platelets 292,000/mm3
Differential significant for 97% Polymorphonuclear lymphocytes
Liver function tests significant for total bilirubin 1.9 mg/dL, direct bilirubin 1.2 mg/dL, AST 60 U/L, ALT 129 U/L, Alkaline Phosphatase 344 U/L
Amylase and lipase within normal limits
Serum chemistries within normal limits
Urinalysis was significant for 5-10 white blood cells per HPF and trace leukocyte esterase
Chest x-ray demonstrated no evidence of cardiopulmonary disease.
Abdominal ultrasound showed no acute process.
Blood cultures were collected and the patient was started on empiric antibiotic therapy with Vancomycin and Cefotaxime. Within 24 hours, all blood cultures were positive with gram stain showing gram positive cocci in pairs and chains. This organism was later speciated as Lancefield group A, beta-hemolytic streptococci (Streptococcus pyogenes).
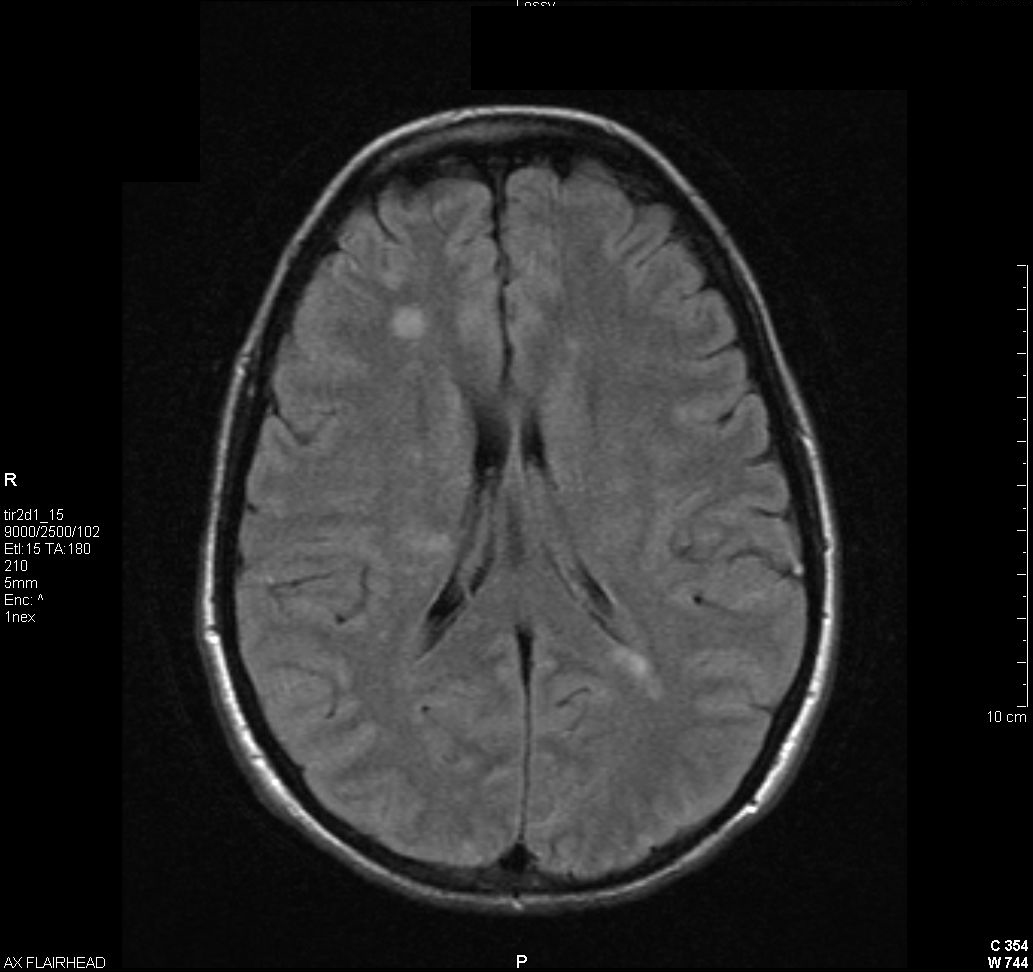
Echocardiography demonstrated a15mm x 10mm mobile, subvalvular vegetation involving the papillary muscles of the posterior mitral valve leaflet. (see video showing mitral valve vegetation) Despite antibiotic treatment, she developed confusion and blurred vision with associated headache and photophobia. An ophthalmologic examination disclosed bilateral uveitis and MRI of the brain demonstrated numerous bihemispheric lesions consistent with septic emboli (figure 1).
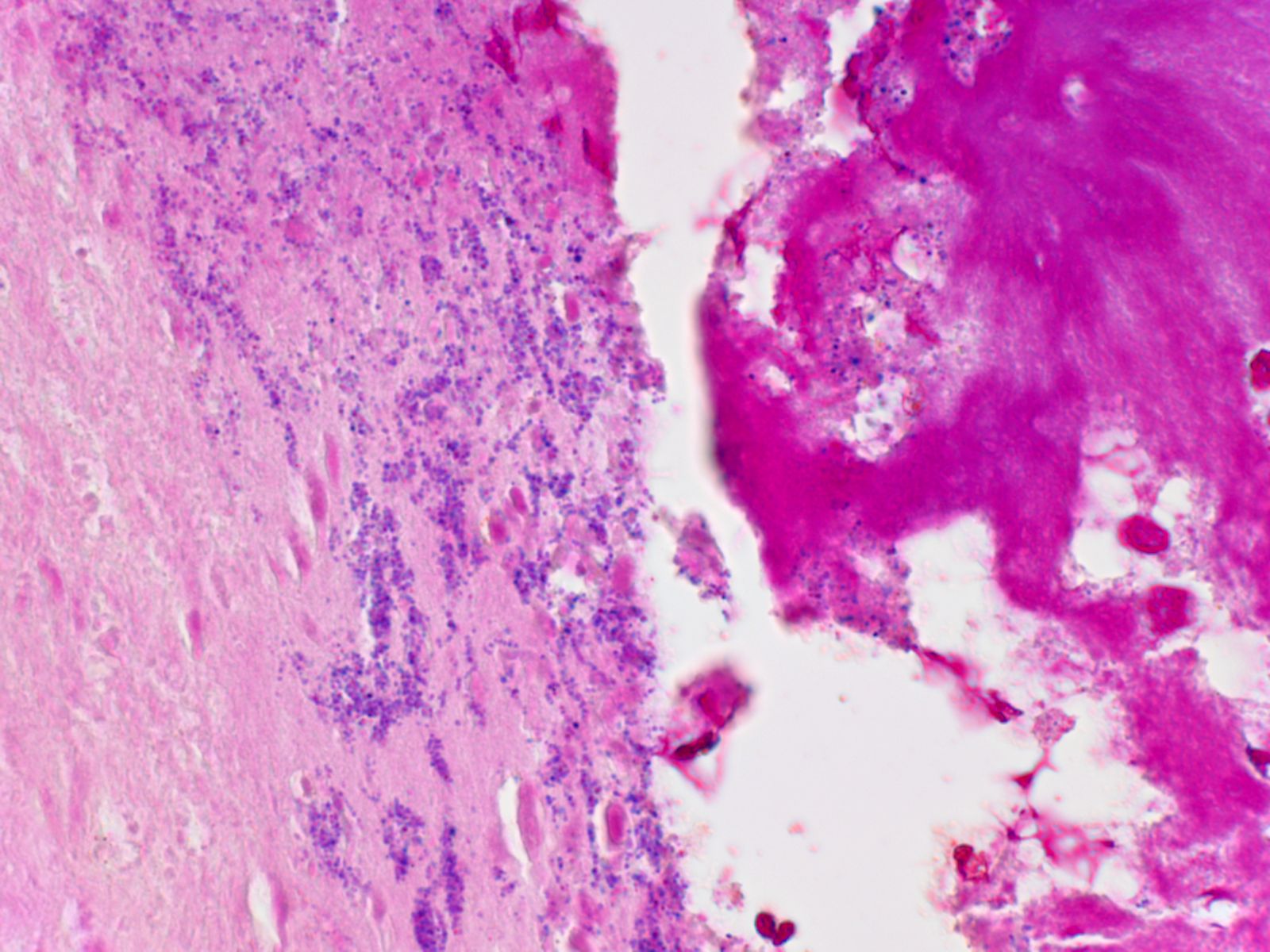
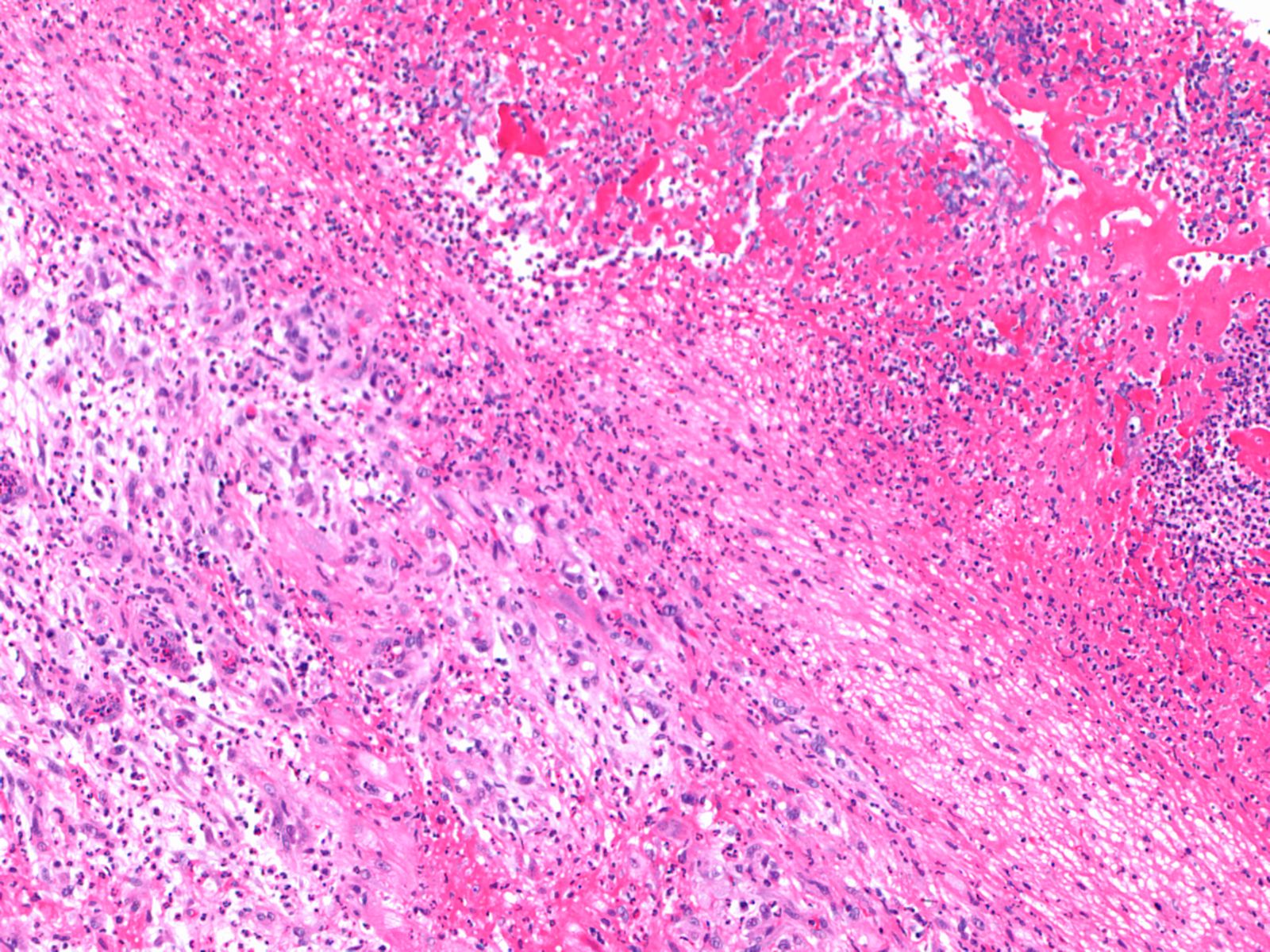
The patient underwent median sternotomy for resection of the vegetation, which was adherent to the papillary muscle, chordae tendinae and posterior wall of the left ventricle, and stained positively for gram positive cocci. (figure 2) Postoperatively, the patient had an uneventful recovery and was discharged home on post-operative day number seven to complete six weeks of intravenous cefotaxime. At the time of follow-up, the patient was found to be doing well with complete resolution of her prior symptoms. Repeat laboratory data, including liver function tests, were entirely within normal limits.
Group A streptococi are characterized by the presence of M proteins, which are the predominant virulence factor associated with invasive infection. It has been demonstrated that streptococcus pyogenes is non-pathogenic when M protein is absent.(1) These finger-like proteins extend through the organism’s protective hyaluronic acid capsule, thus exerting their pathogenic effects while leaving the bacterium protected from the host environment. There are over 150 subtypes of M proteins and classification schemes have been developed to further classify subtypes of group A streptococci based on the characteristics of individual M proteins. There is evidence to suggest that acquired host immunity is specific for individual M protein subtypes, thus providing limited defense against repeated infection.(2) Once inside the host’s circulatory system, M proteins form complexes with fibronogen and adhere to vascular endothelium.(3) After tethering to the endovascular surface, the complexes lead to activation of circulating polymorphnuclear lymphocytes, release of proteolytic enzymes and degradation of vascular endothelium. In this manner, the degraded endothelial surface is thus rendered vulnerable to translocation of the organism into surrounding tissue planes. Once infection has occurred, M protein also functions to protect the invading organism from host defenses. For instance, M protein has been shown to facilitate adhesion to cell surfaces (4) , inhibiting phagocytosis by interfering with opsonization through the complement pathway (5) and even allowing the organism to be internalized within human epithelial cells (6) , thus allowing the organism to evade host defenses.
While group A streptocci are well adapted to invasive soft tissue infection, the organism is perhaps most notorious for the production of superantigens. These potent virulence factors exert a powerful inflammatory effect by binding to MHC class II receptors on circulating T cells, thus prompting the exuberant release of interleukins and cytokines facilitating an exponential cascade of immunologic activity that characterizes streptococcal toxic shock syndrome.(7) This life-threatening condition is characterized by fever, bacteremia, multi-organ failure and widespread desquamative skin lesions. However, the development of streptococcal toxic shock syndrome is relatively infrequent among patients with group A streptococcal bacteremia. In one study, it was found that while streptococcal toxic shock syndrome occurred in only 9% of patients with group A streptococcal bacteremia, it was associated with significant mortality when present.(8)
In addition to prompt surgical intervention, early and appropriate antibiotic therapy is crucial to the effective management of invasive streptococcal disease and toxic shock syndrome. When toxic shock syndrome is suspected, initial empiric therapy should be directed against both Staphylococcus Aureus and Streptococcus Pyogenes, and must account for potential resistance of these organisms to methicillin and erythromycin, respectively. However, once infectious with group A streptococci has been confirmed, the antibiotic regimen of choice is penicillin and clindamycin. This regimen is recommended by the Infectious Disease Society of America (Grade A2).(9 )
While group A streptococcus continues to remains sensitive to b-lactam antibiotics, the bactericidal effects of penicillin have been shown to be less effective in the setting of high organism burden. Studies demonstrating the ineffectiveness of b-lactams alone in the treatment of invasive group A streptococcal infection date back to the early 1950’s when Eagle and colleagues used a murine model to demonstrate that penicillin alone is ineffective in treating group A streptococcal infections with high innoculum size.(10) This phenomenon, which has been referred to as the “inoculum effect”, is thought to be attributable to down-regulated expression of penicillin binding proteins when the organism is in the stationary growth phase, which is achieved more rapidly with a larger bacterial load.(11) A subsequent investigation by Stevens and colleagues expanded upon early work by Eagle to demonstrate that penicillin, clindamycin and erythromycin appear to be equally effective early on in the infectious process with 100% survival across all groups.(12) However, survival rates in this model of invasive streptococcal infection diverge abruptly later in the infectious process, with only 60% survival in the penicillin group, compared with 100% in both the clindamycin and erythromycin groups 12 days after initial inoculation. Furthermore, it was shown that delaying the initiation of antibiotic therapy for as little as 2 hours reduced the survival rates in the penicillin and erythromycin treatment groups to 30% and 70% respectively, while clindamycin remained equally efficacious with 100% survival despite treatment delays. Even when the initiation of clindamycin therapy was delayed for as long 16.5 hours after inoculation, the survival rate remained as high as 70%. The decreased mortality associated with clindamycin use is likely attributable to the direct inhibitory effects of this medication on specific streptococcal pathogenicity and virulence factors. It has been shown that M protein production is suppressed in the presence of clindamycin, thus leading to enhanced opsonization and phagocytosis by polymorphonuclear leukocytes.(13) Use of clindamycin has been shown to result in a greater decrease in Exotoxin production when compared to use of b-lactams.(14, 15) However, while clindamycin has a well-established role in the treatment of invasive group A streptococcal disease, the addition of penicillin is still recommended due to the continued sensitivity of the organism to b-lactam antibiotics and the increasing potential for macrolide resistance among group A streptocci.(16, 17)
Appropriate suspicion and early recognition of invasive streptococcal disease is crucial for effective management of invasive group A streptococcal infection. The Centers for Disease Control and Prevention maintain comprehensive epidemiologic data regarding group A streptococcal infection as part of the Active Bacterial Core Surveillance (ABCS) report. The most recent data from the CDC estimate that 12,000 cases of invasive group a streptococcal infection occur annually with 1,600 associated deaths (mortality rate of 13.3%).(18) Available data suggest a bi-modal age distribution, with highest rates occurring among infants and the elderly.(18) However, among IV drug users a striking increase in the incidence of group A streptococcal bacteremia has been reported in the second and third decades of life.(8 ) Available case series have shown that group A streptococcus is a relatively rare isolate from the blood, representing approximately 1% of all bacteremias.(8) Animal models have shown that group A streptococcal bacteremia may persist for weeks after inoculation, and can be accelerated by minor muscle and soft tissue trauma.(19)
While it is important to recognize that a large proportion of invasive group A streptococcal infections have no known portal of entry (20), national data from the CDC has demonstrated that when a site of entry is known, cellulitis is the most common (31.5%) localized infection associated with invasive group A streptococcal infection, followed by pneumonia (17%) and necrotizing fasciitis (6.6%).(18 ) A similar distribution of localized infections has been described among ICU patients with invasive group A streptococcal infection.(21 ) Among IV drug users, an identifiable cutaneous portal of entry such as suppurative phlebitis or skin abscess is present in the majority of cases and severe skin infections have been associated with higher mortality rates.(8)
Among the various manifestations of invasive group a streptococcal infection, endocarditis is an exceedingly rare complication. A nationwide retrospective study in France identified only 7 cases associated with group A streptococcus over a 10 year period. Interestingly, among those patients with group A streptococcal bacteremia, septic embolization is common and often occurs without echocardiographic evidence of endocarditis.(8) When endocardial involvement is present, group A streptococci often involve otherwise normal native heart valves and has been shown to have a 21% mortality rate.(22) Therefore, although rare, endocarditis is often difficult to differentiate from bacteremia, thus creating a therapeutic dilemma regarding the type and duration of therapy.
Among patients with invasive group A streptococcal infection, the need for ICU care is common. A prospective observational study of ICU patients with invasive group A streptococcal infection demonstrated that progressive multi-organ failure such as ARDS, renal failure requiring replacement therapy, hepatic dysfunction, neurologic dysfunction and coagulopathy was commonly seen in advanced disease states.(21) Among ICU patients with invasive group A streptococcal disease, overall mortality is high (40%) and often occurs less than 7 days following ICU admission. Not surprisingly, risk of death among ICU patients has been shown to be associated with higher Acute Physiology And Chronic Health Evaluation (APACHE II) scores score and number of dysfunctional organs and the presence of streptococcal toxic shock syndrome.
Intravenous immunoglobulin (IVIg) is a therapy that has been extensively investigated in the context of invasive group A streptococcal disease, particularly streptococcal toxic shock syndrome. The rationale for the use of IVIg is based upon the observation that antibodies directed against specific group A streptococcal virulence factors are present at lower levels in patients with invasive disease compared to controls.(23) It has also been shown that circulating levels of anti-M protein antibodies are significantly increased in patients with streptococcal toxic shock syndrome following IVIg therapy, thus leading to opsonization and clearance of the organism.(24) Numerous case reports published over the past several decades have suggested that patients with invasive streptococcal disease have improved outcomes when treated with IVIg.(25, 26) However, a larger observational study by Kaul and colleagues in 1999 demonstrated a marked reduction in mortality among patients with streptococcal toxic shock syndrome who were treated with IVIg when compared to controls at 30 days (34% vs. 67%).(27) Furthermore, analysis of serum from both treated patients and controls demonstrated a significant reduction in T-cell mediated production of IL-6 and TNF-a. A subsequent randomized, double-blind, placebo-controlled trial demonstrated a three-fold reduction in 28 day mortality (36% vs. 10%) among patients treated with IVIg but failed to achieve statistical significance, possibly due to small sample size with 10 and 11 patients in the treatment and placebo arms respectively.(28) Interestingly however, a prospective observational study of ICU patients with invasive streptococcal infection found no association between the use of IVIg and survival.(21) Citing inconsistencies in commercially available IVIg and the need for more conclusive investigation regarding the role of IVIg in treating invasive group A streptococcal infection, the Infectious Disease Society of America offers a grade 2B recommendation for the use of IVIg (Moderate evidence to support a recommendation for use; should generally be offered).(9)
There has been extensive research investigating the potential use of vaccines to prevent group a streptococcal infection. Among other streptococcal antigens, M protein has been investigated as a potential vaccine target. The variability among M protein subtypes and the specificity of acquired host immunity pose a challenge to vaccine development. However, a 26 valent vaccine targeting the predominant M protein epitopes found in the United States and Europe was shown to induce host antibodies that were capable of opsonizing targeted M protein subtypes as well as several subtype variants not represented.(29) This vaccine has been evaluated in phase I and phase II human clinical trials and has been found to be safe and effective in inducing antibody production and subsequent opsonization.(30) While these results are certainly encouraging, vaccine strategies to prevent group A streptococcal infection remain investigational.
References
Brooks G, Butel J, Morse S. Jawetz, melnick, & adelberg's medical microbiology. New York: McGraw Hill; 2004.
de Malmanche SA, Martin DR. Protective immunity to the group a streptococcus may be only strain specific. Med Microbiol Immunol 1994;183(6):299-306
Herwald H, Cramer H, Morgelin M, Russell W, Sollenberg U, Norrby-Teglund A, Flodgaard H, Lindbom L, Bjorck L. M protein, a classical bacterial virulence determinant, forms complexes with fibrinogen that induce vascular leakage. Cell 2004;116(3):367-379.
Frick IM, Schmidtchen A, Sjobring U. Interactions between m proteins of streptococcus pyogenes and glycosaminoglycans promote bacterial adhesion to host cells. Eur J Biochem 2003;270(10):2303-2311
Peterson PK, Schmeling D, Cleary PP, Wilkinson BJ, Kim Y, Quie PG. Inhibition of alternative complement pathway opsonization by group a streptococcal m protein. J Infect Dis 1979;139(5):575-585.
Greco R, De Martino L, Donnarumma G, Conte MP, Seganti L, Valenti P. Invasion of cultured human cells by streptococcus pyogenes. Res Microbiol 1995;146(7):551-560.
Norrby-Teglund A, Thulin P, Gan BS, Kotb M, McGeer A, Andersson J, Low DE. Evidence for superantigen involvement in severe group a streptococcal tissue infections. J Infect Dis 2001;184(7):853-860.
Bernaldo de Quiros JC, Moreno S, Cercenado E, Diaz D, Berenguer J, Miralles P, Catalan P, Bouza E. Group a streptococcal bacteremia. A 10-year prospective study. Medicine (Baltimore) 1997;76(4):238-248.
Stevens DL, Bisno AL, Chambers HF, Everett ED, Dellinger P, Goldstein EJ, Gorbach SL, Hirschmann JV, Kaplan EL, Montoya JG, et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis 2005;41(10):1373-1406
Eagle H. Experimental approach to the problem of treatment failure with penicillin. I. Group a streptococcal infection in mice. Am J Med 1952;13(4):389-399.
Stevens DL, Yan S, Bryant AE. Penicillin-binding protein expression at different growth stages determines penicillin efficacy in vitro and in vivo: An explanation for the inoculum effect. J Infect Dis 1993;167(6):1401-1405.
Stevens DL, Gibbons AE, Bergstrom R, Winn V. The eagle effect revisited: Efficacy of clindamycin, erythromycin, and penicillin in the treatment of streptococcal myositis. J Infect Dis 1988;158(1):23-28.
Gemmell CG, Peterson PK, Schmeling D, Kim Y, Mathews J, Wannamaker L, Quie PG. Potentiation of opsonization and phagocytosis of streptococcus pyogenes following growth in the presence of clindamycin. J Clin Invest 1981;67(5):1249-1256.
Sriskandan S, McKee A, Hall L, Cohen J. Comparative effects of clindamycin and ampicillin on superantigenic activity of streptococcus pyogenes. J Antimicrob Chemother 1997;40(2):275-277.
Coyle EA, Cha R, Rybak MJ. Influences of linezolid, penicillin, and clindamycin, alone and in combination, on streptococcal pyrogenic exotoxin a release. Antimicrob Agents Chemother 2003;47(5):1752-1755.
Richter SS, Heilmann KP, Dohrn CL, Beekmann SE, Riahi F, Garcia-de-Lomas J, Ferech M, Goossens H, Doern GV. Increasing telithromycin resistance among streptococcus pyogenes in europe. J Antimicrob Chemother 2008;61(3):603-611.
Mazzariol A, Koncan R, Bahar G, Cornaglia G. Susceptibilities of streptococcus pyogenes and streptococcus pneumoniae to macrolides and telithromycin: Data from an italian multicenter study. J Chemother 2007;19(5):500-507.
Centers for Disease Control and Prevention. 2009. Active bacterial core surveillance report, emerging infections program network, group a streptococcus, 2008. Available from: http://www.cdc.gov/abcs/reports-findings/survreports/gas08.pdf .
Seki M, Saito M, Iida K, Taniai H, Soejima T, Nakayama H, Yoshida S. Onset of streptococcal toxic shock syndrome is accelerated by bruising in a mouse model. Microb Pathog 2008;44(4):339-343.
Stevens DL. Invasive group a streptococcus infections. Clin Infect Dis 1992;14(1):2-11.
Mehta S, McGeer A, Low DE, Hallett D, Bowman DJ, Grossman SL, Stewart TE. Morbidity and mortality of patients with invasive group a streptococcal infections admitted to the icu. Chest 2006;130(6):1679-1686.
Burkert T, Watanakunakorn C. Group a streptococcus endocarditis: Report of five cases and review of literature. J Infect 1991;23(3):307-316.
Basma H, Norrby-Teglund A, Guedez Y, McGeer A, Low DE, El-Ahmedy O, Schwartz B, Kotb M. Risk factors in the pathogenesis of invasive group a streptococcal infections: Role of protective humoral immunity. Infect Immun 1999;67(4):1871-1877.
Basma H, Norrby-Teglund A, McGeer A, Low DE, El-Ahmedy O, Dale JB, Schwartz B, Kotb M. Opsonic antibodies to the surface m protein of group a streptococci in pooled normal immunoglobulins (ivig): Potential impact on the clinical efficacy of ivig therapy for severe invasive group a streptococcal infections. Infect Immun 1998;66(5):2279-2283.
Barry W, Hudgins L, Donta ST, Pesanti EL. Intravenous immunoglobulin therapy for toxic shock syndrome. Jama 1992;267(24):3315-3316.
Lamothe F, D'Amico P, Ghosn P, Tremblay C, Braidy J, Patenaude JV. Clinical usefulness of intravenous human immunoglobulins in invasive group a streptococcal infections: Case report and review. Clin Infect Dis 1995;21(6):1469-1470.
Kaul R, McGeer A, Norrby-Teglund A, Kotb M, Schwartz B, O'Rourke K, Talbot J, Low DE. Intravenous immunoglobulin therapy for streptococcal toxic shock syndrome--a comparative observational study. The canadian streptococcal study group. Clin Infect Dis 1999;28(4):800-807.
Darenberg J, Ihendyane N, Sjolin J, Aufwerber E, Haidl S, Follin P, Andersson J, Norrby-Teglund A. Intravenous immunoglobulin g therapy in streptococcal toxic shock syndrome: A european randomized, double-blind, placebo-controlled trial. Clin Infect Dis 2003;37(3):333-340.
Dale JB, Penfound T, Chiang EY, Long V, Shulman ST, Beall B. Multivalent group a streptococcal vaccine elicits bactericidal antibodies against variant m subtypes. Clin Diagn Lab Immunol 2005;12(7):833-836.
McNeil SA, Halperin SA, Langley JM, Smith B, Warren A, Sharratt GP, Baxendale DM, Reddish MA, Hu MC, Stroop SD, et al. Safety and immunogenicity of 26-valent group a streptococcus vaccine in healthy adult volunteers. Clin Infect Dis 2005;41(8):1114-1122.
The American Thoracic Society improves global health by advancing research, patient care, and public health in pulmonary disease, critical illness, and sleep disorders. Founded in 1905 to combat TB, the ATS has grown to tackle asthma, COPD, lung cancer, sepsis, acute respiratory distress, and sleep apnea, among other diseases.
AMERICAN THORACIC SOCIETY 25 Broadway New York, NY 10004 United States of America