Reviewed By Environmental & Occupational Health Assembly
Submitted by
Leslie Israel DO, MPH
Associate Clinical Professor
Department of Medicine, Division of Occupational and Environmental Medicine
University of California, Irvine
Irvine, California
Thomas Kim MD, MPH
Medical Officer/Epidemic Intelligence Service Officer
California Department of Public Health
Centers for Disease Control and Prevention
Janice Prudhomme DO, MPH
Occupational Health Branch, Hazard Evaluation System and Information Service
California Department of Public Health
Rachel Bailey DO, MPH
Medical Officer
National Institute for Occupational Safety and Health, Division of Respiratory Disease Studies
Centers for Disease Control and Prevention
Philip Harber MD, MPH
Professor, Chief
Department of Family Medicine, Division of Occupational and Environmental Medicine
University of California, Los Angeles
Submit your comments to the author(s).
History
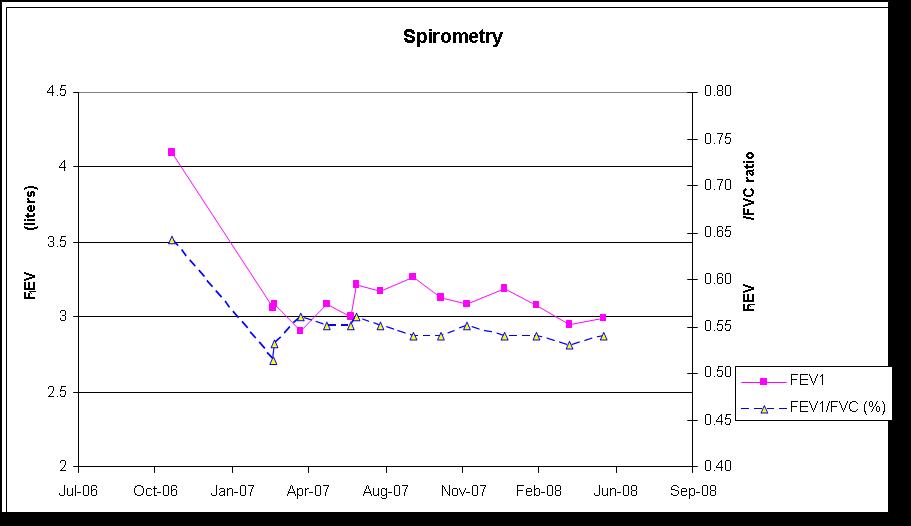
A food flavoring manufacturing facility offers periodic workplace spirometry testing to its employees. The testing is done by medical professionals at the worksite without charge to the employees. Results for one employee are shown in Table 1.
|
Measurements |
10/31/06 |
3/13/07 |
Repeated on 3/14/07 |
||
|
Pre-BD |
Post-BD* |
Pre-BD |
Post-BD* |
||
|
FVC (L) |
6.38 |
5.96 |
5.82 |
5.77 |
5.67 |
|
FVC Percent predicted |
113.5% |
106.2% |
102.8% |
||
|
FEV1 (L) |
4.10 |
3.06 |
3.09 |
3.02 |
3.02 |
|
FEV1 Percent predicted |
86.5% |
64.5% |
63.7% |
||
|
FEV1/FVC† |
64.4% |
51.3% |
53.0% |
52.3% |
53.3% |
Table 1. Spirometry findings during medical surveillance at workplace.
*No significant improvement in FVC or FEV1 with bronchodilator. †Lower limit of normal: 89.2% FVC, forced vital capacity; FEV1, forced expiratory volume in the first second of exhalation; L, liter; BD, bronchodilator; %, percent.
The employee, a 25-year-old man assigned to mixing food flavorings, is found to have an abnormal spirogram during routine workplace medical surveillance. He is referred for evaluation to an occupational environmental medicine (OEM) physician in March 2007. The employee reports his general health status is good and denies respiratory symptoms.
The OEM physician obtains an occupational history as follows: No prior occupational history of direct exposures to chemicals or other toxic agents. From 1995 to 2000, he fed animals (primarily cattle) on a farm in Mexico, and from 2001 to 2004, he worked in the warehouse and shipping departments at various companies. In December 2004, he began working for a temporary agency that placed him at the food flavoring plant. In June 2005, he was hired by the food flavoring company and worked in flavoring production. He reportedly used a dust mask on occasion. In February 2006, he began using a half-facepiece air-purifying respirator. In September 2006, he was given a full-facepiece respirator. Fit-testing had not been done on the half-or full-facepiece respirators until January 2007 when he was quantitatively fit-tested for a full-facepiece respirator.
He denies any prior medical history of pulmonary disease or chronic medical conditions. He denies any allergies. He takes no prescribed or over-the-counter medications. His family history is negative for pulmonary disease. He reports occasional cigarette smoking for one year in 2004 - 2005.
He does not have any pets in his home. He denies any hobbies or second jobs (such as auto repair, construction, or other tasks that would involve possible exposures to pulmonary toxicants). His leisure time activities include: family gatherings, jogging and playing soccer.
Figures

Figure 1: High-resolution computed tomography (HRCT) of chest performed on April 17, 2007.
References
- National Toxicology Program (NTP). Chemical information review document for artificial butter flavoring and constituents diacetyl [CAS no. 431-03-8] and acetoin [CAS no. 513-86-0]. Integrated Laboratory Systems, Inc. Research Triangle Park, NC; 2007.
- Harber P, Saechao K, Boomus C. Diacetyl-induced lung disease. Toxicol Rev 2006; 25:261-272.
- van Rooy FG, Rooyackers JM, Prokop M, Houba R, Smit LA, Heederik DJ. Bronchiolitis obliterans syndrome in chemical workers producing diacetyl for food flavorings. Am J Respir Crit Care Med 2007;176:498-504.
- Centers for Disease Control. Fixed obstructive lung disease among workers in the flavor-manufacturing industry – California, 2004–2007. MMWR Morb Mortal Wkly Rep 2007;56:389–393.
- Kanwal R. Bronchiolitis obliterans in workers exposed to flavoring chemicals. Curr Opin Pulm Med 2008;14:141-146.
- Hubbs AF, Battelli LA, Goldsmith WT, Porter DW, Frazer D, Friend S, Schwegler-Berry D, Mercer RR, Reynolds JS, Grote A, Castranova V, Kullman G, Fedan JS, Dowdy J, Jones WG. Necrosis of nasal and airway epithelium in rats inhaling vapors of artificial butter flavoring. Toxicol Appl Pharmacol 2002;185:128–135.
- Hubbs AF, Battelli LA, Mercer RR, Kashon M, Friend S, Schwegler-Berry D, Goldsmith WT. Inhalation toxicity of the flavoring agent, diacetyl (2,3-butanedione), in the upper respiratory tract of rats. Toxicol Sci 2004;78 Suppl 1:438–439.
- Hubbs AF, Goldsmith WT, Kashon ML, Frazer D, Mercer RR, Battelli LA, Kullman GL, Schwegler-Berry D, Friend S, Castranova V. Respiratory toxicologic pathology of inhaled diacetyl in Sprague-Dawley rats. Toxicol Pathol 2008;36:330–344.
- Morgan DL, Flake G, Kirby PJ, Palmer SM. Respiratory toxicity of diacetyl in C57BL/6 mice. Toxicol Sci 2008;103:169–180.
- Frank AL. Approach to the patient with an occupational or environmental illness. Prim Care 2000;27:877-894.
- ATSDR (Agency for Toxic Substances and Disease Registry). Case studies in environmental medicine: taking an exposure history. 2008 [accessed 2009 Mar 02] Available from: http://www.atsdr.cdc.gov/csem/exphistory/ehcover_page.html.
- CDPH (California Department of Public Health). Medical surveillance for flavorings-related lung disease among flavor manufacturing workers in California. Occupational Health Branch, California Department of Public Health; 2007. Available from: http://www.cdph.ca.gov/programs/ohb/Pages/FlavoringsPubs.aspx.
- Balmes JR. Occupational lung diseases. In: LaDou J, editor. Current occupational & environmental medicine, 4th ed. McGraw-Hill Professional 2007. pp. 310 – 312.
- Langmuir AD. The surveillance of communicable diseases of national importance. N Engl J Med 1963;268:182-191.
- Levy BS, Wegman DH, Halperin WE. Recognizing occupational disease and injury. In:Levy BS, Wegman Dh, editors. Occupational health: recognizing and preventing work-related disease and injury. Philadelphia: Lippincott William & Wilkins, 2000. pp. 4:99-144.
- Occupational Safety and Health Administration (OSHA). OSHA medical screening and surveillance standards. 2007, [accessed 2009 Feb 25]. Available from: http://www.osha.gov/SLTC/medicalsurveillance/standards.html.
- Centers for Disease Control. NIOSH alert: preventing lung disease in workers that use or make flavorings. Cincinnati, OH: US Department of Health and Human Services, CDC, National Institute for Occupational Safety and Health; 2003. (DHHS [NIOSH] publication no. 2004-110.) Available from: http://www.cdc.gov/niosh/docs/2004-110/.
- National Institute for Occupational Safety and Health(NIOSH). NIOSH safety and health topic: flavoring-related lung disease. 2008 [accessed 2008 Mar 02]. Available from: http://www.cdc.gov/niosh/topics/flavorings.
- Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, vand der Grinten CPM, Gustafsson P, Jensen R, Johnson DC, MacIntyre, N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J; ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J 2005;26:319 – 338.
- Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. A J Respir Crit Care Med 1999;159:179-187.
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948-968.
- National Institute for Occupational Safety and Health (NIOSH). NIOSH safety and health topic: spirometry training course. 2009 [accessed 2009 Feb 25]. Available from: http://www.cdc.gov/niosh/topics/spirometry.
- Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J; ATS/ERS Task Force. General considerations for lung function testing. Eur Respir J 2005;26:153-161.



{kind=link}