Contributed by Omer Ahmed, MD, and Sairam Parthasarathy, MD, Southern Arizona VA Health Care System and University of Arizona
A 64 y/o male with history of snoring and daytime sleepiness was referred to the sleep clinic. Examination revealed normal blood pressure, normal body habitus, with body mass index of 28 kg/m2. Head and neck examination revealed grade II (Mallampati) throat with no evidence for tonsillar enlargement or nasal obstruction. Cardiovascular and respiratory examination was normal. There were no neurological deficits identified.
The patient underwent an overnight polysomnography which revealed the presence of positional sleep apnea with overall apnea-hypopnea index (AHI) of 12 per hour (supine AHI of 32 per hour) and lowest oxygen saturation of 88% by pulseoximetry. The patient subsequently underwent positive airway pressure (PAP) titration, but failed to tolerate such therapy. He refused mandibular advancement device and preferred to try position therapy using a custom made pillow.
The patient subsequently underwent a research study investigating a novel therapeutic modality for obstructive sleep apnea. Representative tracings from the research polysomnography during wakefulness (A) and non-rapid eye movement (NREM) sleep (B) are shown below. What does the tracing show? What novel therapeutic modality could be responsible for such polysomnographic findings?
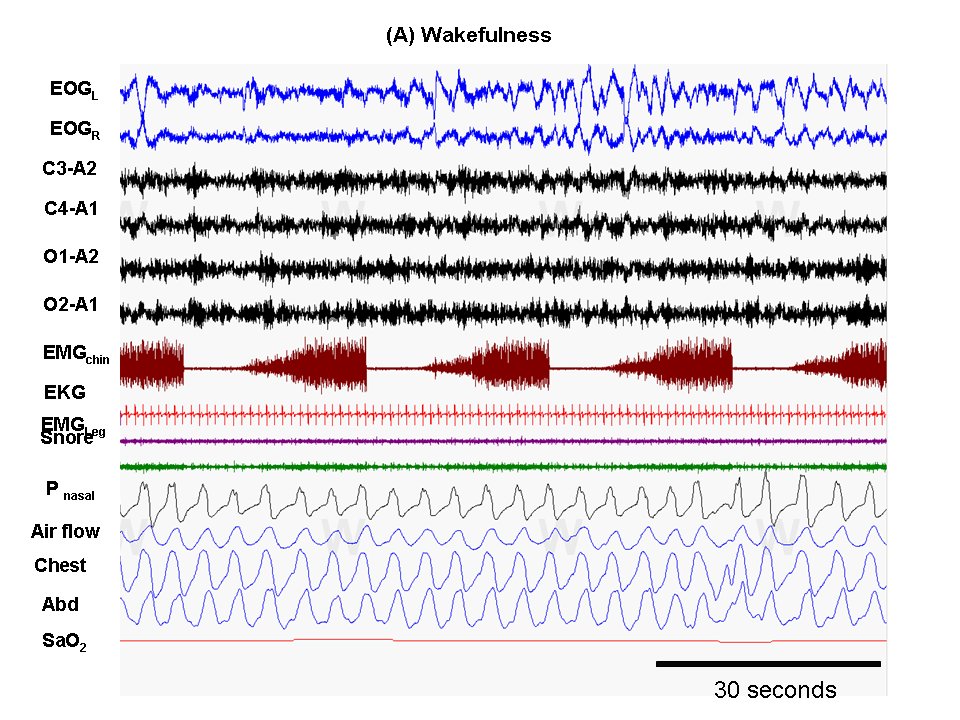

The polysomnographic tracings reveal evidence for repetitive activity in the chin electromyography (EMG) channel. Such activity is dysynchronous with respiration and occurs during wakefulness and sleep. Note that the respiratory tracings during these periods of time are without any respiratory events and the electroencephalographic (EEG) tracings are without arousals from sleep. The measured EMG activity is secondary to genioglossus muscle stimulation through implanted electrodes aimed at improving upper airway patency and ameliorating sleep-disordered breathing. A comparison montage of demonstrating the occurrence of events of sleep-disordered breathing when the device was turned off is shown in figure C.
Stimulation of genioglossus muscle has been variably attempted by implanting electrodes directly into the genioglossal musculature1,2; stimulating the hypoglossal and genioglossal nerves3; by transcutaneous stimulation of the hyoglossus and genioglossus muscle4; or intraoral stimulation of the genioglossal muscle5. Previous studies have demonstrated that electrical stimulation of genioglossus has achieved reduction in critical closing pressure (Pcrit) of the upper airway, reduction of AHI, and is tolerated during sleep6,7. However, such stimulation of the upper airway muscles does not appear to achieve the same efficacy as PAP therapy in correcting events of sleep-disordered breathing8. The inability of upper airway muscle stimulation to completely correct upper airway obstruction may be attributable to the complex interplay of retractor and protrusor muscles of the tongue, hyoglossus, and styloglossus and also to other upper airway collapsing forces that are not corrected by such muscle stimulation5.
References
- Decker MJ, Haaga J, Arnold JL, Atzberger D, Strohl KP. Functional electrical stimulation and respiration during sleep. J Appl Physiol. 1993;75:1053-61.
- Schwartz AR, Eisele DW, Hari A, Testerman R, Erickson D, Smith PL. Electrical stimulation of the lingual musculature in obstructive sleep apnea. J Appl Physiol. 1996;81:643-52.
- Eisele DW, Smith PL, Alam DS, Schwartz AR. Direct hypoglossal nerve stimulation in obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 1997;123:57-61.
- Hillarp B, Rosén I, Wickström O. Videoradiography at submental electrical stimulation during apnea in obstructive sleep apnea syndrome. A case report. Acta Radiol. 1991;32:256-9.
- Oliven A, Schnall RP, Pillar G, Gavriely N, Odeh M. Sublingual electrical stimulation of the tongue during wakefulness and sleep. Respir Physiol. 2001;127:217-26.
- Oliven A, O'Hearn DJ, Boudewyns A, Odeh M, De Backer W, van de Heyning P, Smith PL, Eisele DW, Allan L, Schneider H, Testerman R, Schwartz AR. Upper airway response to electrical stimulation of the genioglossus in obstructive sleep apnea. J Appl Physiol. 2003;95:2023-9.
- Oliven R, Tov N, Odeh M, Gaitini L, Steinfeld U, Schwartz AR, Oliven A. Interacting effects of genioglossus stimulation and mandibular advancement in sleep apnea. J Appl Physiol. 2009;106:1668-73.
- Schwartz AR, Bennett ML, Smith PL, De Backer WA, Hedner J, Boudewyns A, Van de Heyning PH, Ejnell H, Hochban W, Knaack L, Podszus T, Penzel T, Peter JH, Goding GS, Erickson DJ, Testerman R, Ottenhoff F, and Eisele DW. Therapeutic electrical stimulation of the hypoglossal nerve in obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 127: 1216-1223, 2001.
- Oliven A, Odeh M, Geitini L, Oliven R, Steinfeld U, Schwartz AR, Tov N. Effect of coactivation of tongue protrusor and retractor muscles on pharyngeal lumen and airflow in sleep apnea patients. J Appl Physiol. 2007;103:1662-8.



