William Beckett MD
University of Rochester
School of Medicine and Dentistry
Michael Kallay
Pulmonary and Critical Care Division
University of Rochester
School of Medicine and Dentistry
Akshay Sood, MD, MPH
Southern Illinois University
School of Medicine
Zhengfa Zuo, PhD
Harvard School of Public Health
and
Donald Milton MD, MPH
University of Massachusetts
Lowell MA
Case presentation:
A 57-year-old nonsmoking auto-parts machine operator presented with shortness of breath on exertion, cough, fatigue, and chest congestion.
In his job he operated a machine that cut metal parts, continuously lubricated by a spray of metalworking fluid (Figure 1) that was collected and recycled through large tanks holding more than 1,000 gallons of fluid.
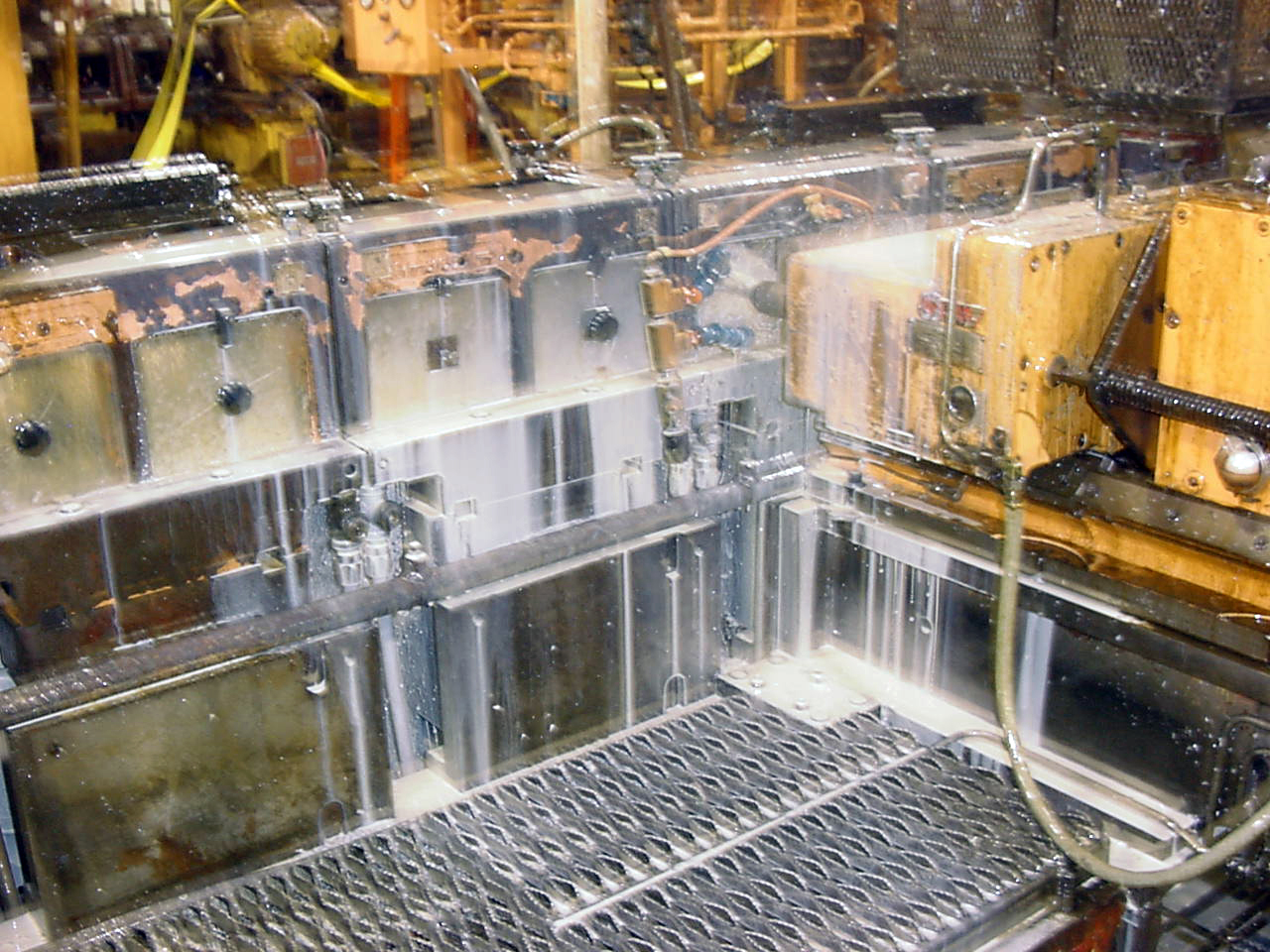
Figure 1. Machine similar to the one operated by this patient. Machine cuts metal parts, and cutting tools are lubricated with a lipid-water solution which cools the friction points and carries away small metal chips.
On physical examination he was afebrile. There were no adventitious breath sounds or changes to percussion. There was no digital clubbing. A chest radiograph showed bilateral increased interstitial markings, and he was treated with empiric antibiotics on two occasions. Symptoms were worse after work, and occupational asthma was suspected, but a trial of bronchodilators was not effective in relieving symptoms. Spirometry was performed in the company medical department just before and after a five-day work week with no change. His physician recommended removing him from exposure to metal working fluids, but the employer medical department misinterpreted this as meaning that the patient had chronic obstructive pulmonary disease, and did not follow the work restrictions for long.
Referral to a pulmonary specialist led to additional testing. Pulmonary function tests are shown (Table 1), and a carbachol challenge was negative.
Table 1
|
FEV1 (% predicted) |
FVC (% predicted) |
DLCO (% predicted) |
O2 Saturation (Rest) |
O2 Saturation (Exercise) |
|
2.52 (89) |
3.14 (89) |
9.4 (44) |
92% |
89% |
A thin-section computed tomography (CT) scan of the chest (Figure 2) showed "ground glass" opacities indicating interstitial lung disease, and mild bronchiectasis.
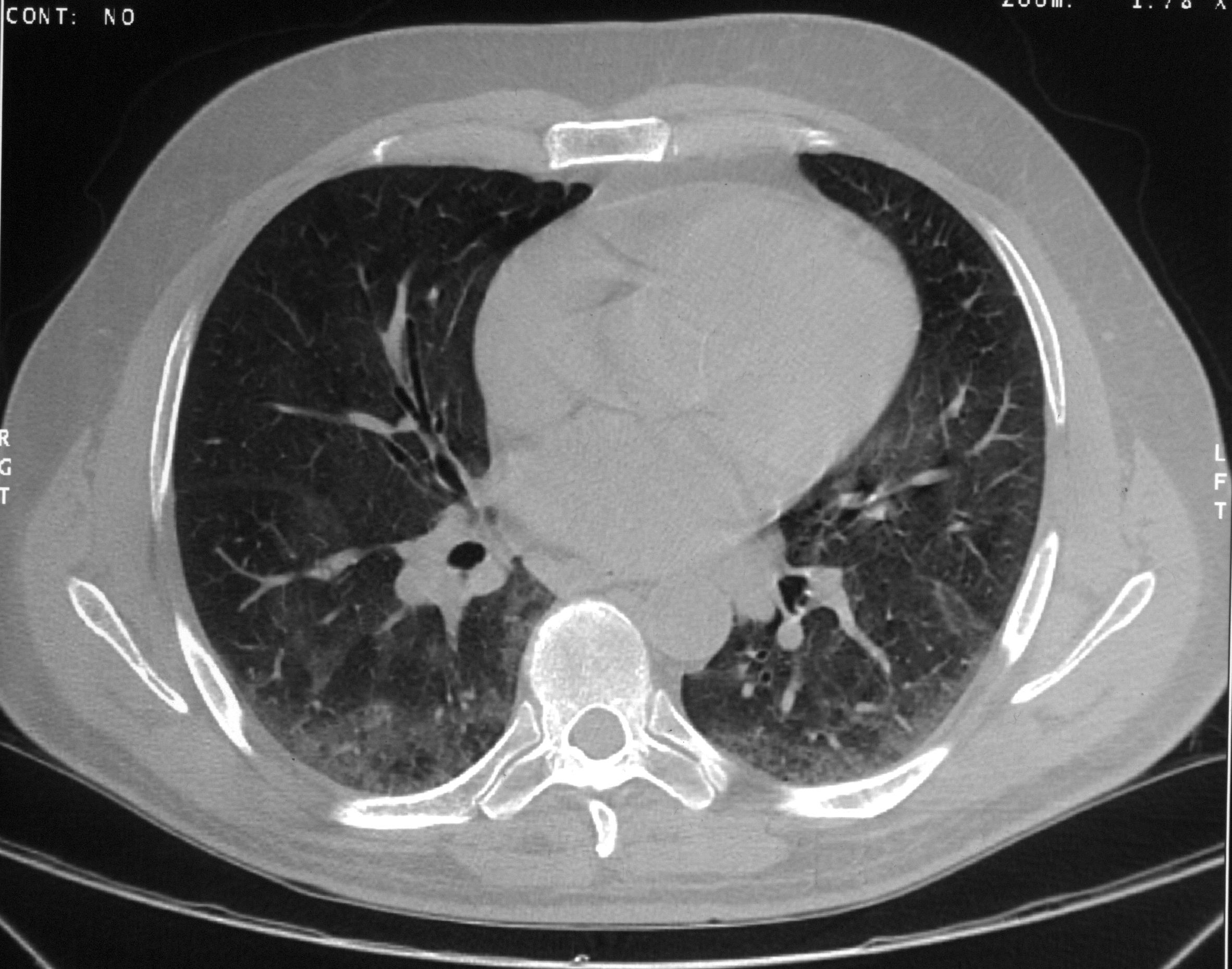
Figure 2: Thin layer CT scan of the chest showing patchy areas of increased interstitial markings.
Bronchial alveolar lavage showed 90% lymphocytes and 10% macrophages in alveolar lining fluid, with negative smear and culture for acid fast bacilli (mycobacteria) and fungi. A transbronchial lung biopsy (Figure 3) showed interstitial chronic inflammation and collections of epithelioid cells suggestive of granulomas with negative stains for acid-fast bacilli and fungus. Serum-precipitating antibodies to a standard panel of nine substances, including bacteria, several fungi, and pigeon serum, were all negative.
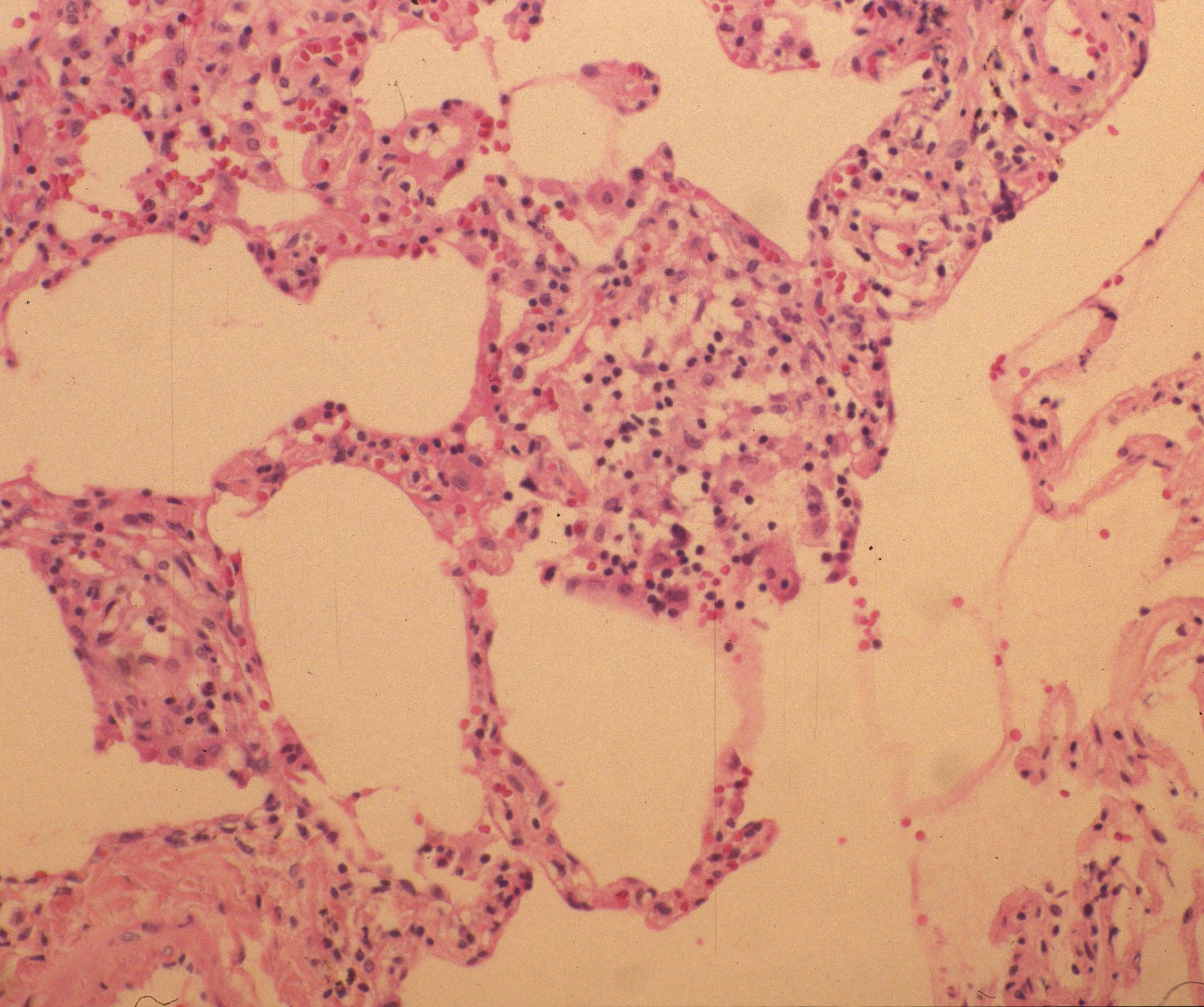
Figure 3. Trans-bronchial biopsy of lung showing interstitial changes and lymphocytic inflammation.
Samples of metalworking fluid which were obtained for culture from the large reservoir supplying metalworking fluids to the patient's work area grew 1.6 X 105 mycobacteria/mL, which were identified as M. chelonae.
Question 1
What is the most likely diagnosis?
a. Occupational asthma
b. Hypersensitivity pneumonitis
c. Atypical mycobacterial infection
d. Sarcoidosis
e. Usual interstitial pneumonitis
The correct answer is b
Hypersensitivity pneumonitis may be caused by many inhaled workplace and environmental substances. It is an acute or chronic inflammatory interstitial process involving prominently the lung parenchyma, most often with a lymphocytic predominance. The acute form may present to the emergency department with the clinical appearance of infectious pneumonia. Chronic disease may present initially with dyspnea, wheezing, and a clear chest radiograph and be mistaken for asthma, or with a gradual and insidious interstitial pattern that clinically resembles chronic pulmonary fibrosis. Prolonged disease may result in chronic pulmonary scarring and death.
A negative serum precipitating antibody panel for hypersensitivity pneumonitis is common in the presence of disease, and does not exclude the diagnosis. Most commercially available panels test for precipitins to approximately 10 common causes of hypersensitivity pneumonitis, but there are many more causes of this disease which are not included in these panels. The panel this patient was tested to did not include precipitins for the mycobacterium isolated from the fluid. Thus serum precipitins can confirm exposure to one or more specific antigens, but may have limited usefulness in the diagnosis of hypersensitivity pneumonitis.
Question 2
What is the likely causative agent for this patient's disease?
a. Steel particles
b. Bird droppings in the rafters of the building
c. Components of the metal working fluid
d. Thermophilic actinomyces
e. Beryllium
The correct answer is c.
Metal working fluids reduce friction and heat in the machining of metal parts, and are normally aerosolized into small droplets which are easily inhaled and retained in the alveoli. These materials are routinely used in high volumes in metal parts manufacturing world wide. Typical use can result in heavy inhalation exposures to machine operators, unless active measures are taken to control air levels.
Metal working fluids comprising of a mixture of lipids and water, serve as a ready culture medium and are always contaminated by microbial growth. Standard usage is to add microbicides to the mixture to maintain the optimal industrial characteristics, but microbicides only reduce the bacterial count.
A number of outbreaks of hypersensitivity pneumonitis have been reported among workers exposed to aerosols of metal working fluids. [1, 2, 3, 4]. In some, disease was associated with mixed bacterial flora growing in the lipid/water mixture of the metal working fluid. In other outbreaks, a non-tuberculous mycobacterium, Mycobacterium Immunogenem [5] was isolated from the fluid.
Question 3
What intervention or interventions are most likely to be effective in this patient?
a. Cyclophosphamide or azathioprine.
b. Inhaled corticosteroids
c. Mycophenylate mofitil
d. Removal from exposure and systemic corticosteroids
e. Antituberculous chemotherapy
The correct answer is d.
Removal from exposure is the most important intervention in hypersensitivity pneumonitis. This may bring about complete resolution, or in chronic cases may prevent further progression of disease. In patients with the acute form of HP, with fever, dyspnea and elevated white cell count, a short course of systemic corticosteroids may bring about a more rapid resolution of the acute episode.
Occupational exposure to metal working fluids has also been associated with respiratory symptoms, bronchitis, asthma, and hard metal pulmonary disease from cobalt dissolved in the fluid. Health recommendations for prevention of the non-hypersensitivity health effects of metal working fluids have been published by the Centers for Disease Control and Prevention [6].
References
- Bernstein D, Lummus Z, Santilli G, Siskosky J, Bernstein I. Machine operator's lung. A hypersensitivity pneumonitis disorder associated with exposure to metal working fluid aerosols. Chest 1995; 108:636-641.
- Centers for Disease Control and Prevention. Respiratory illness in workers exposed to metalworking fluid contaminated with nontuberculous mycobacteria--Ohio, 2001. MMWR Morbid Mortal Wkly Rep 2002; 51:349-352. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5116a4.htm
- Kreiss K, Cox-Gaenser J. Metalworking fluid-associated hypersensitivity pneumonitis: a workshop summary. Am J Indust Med 1997;32:423-432.
- Bracker A, Storey E, Yang C, Hodgson MJ. An outbreak of hypersensitivity pneumonitis at a metalworking plant: a longitudinal assessment of interventional effectiveness. Appl Occup Environ Hyg 2003; 18:96-108.
- Brown-Elliott BA, Wallace RJ Jr. Clinical and taxonomic status of pathogenic nonpigmented or late-pigmenting rapidly growing mycobacteria. Clin Microbiol Rev 2002; 15: 716-746.
- CDC. Criteria for a Recommended Standard: Occupational Exposure to Metalworking Fluids. NIOSH 98-102. 1998. Atlanta, GA: Centers for Disease Control and Prevention.
Acknowledgement: this case was originally published by the US National Institute for Environmental Health Sciences in Environmental Health Perspectives and is reproduced in shortened form with permission of the publisher.


