Reviewed By Critical Care Assembly
Submitted by
Haytham Adada, MD, MBA, FACP
Fellow
Pulmonary and Critical Care department
East Tennessee State University
Tennessee
Souheil Abdel Nour, MD
Fellow
Pulmonary and Critical Care department
East Tennessee State University
Tennessee
Aaysha Kapila, MD
Resident
Internal Medicine
East Tennessee State University
Tennessee
Ryland Byrd, MD, FCCP
Professor
Pulmonary and Critical Care department
East Tennessee State University
Tennessee
Thomas Roy, MD, FCCP
Program director, Professor
Pulmonary and Critical Care department
East Tennessee State University
Tennessee
Submit your comments to the author(s).
History
A 69 year-old woman with a history of coronary artery disease presents with increased shortness of breath and prominent edema of her lower extremities. She also reports a productive cough with pink frothy sputum, but no evident hemoptysis. She denies experiencing orthopnea, paroxysmal nocturnal dyspnea or any other symptoms consistent with congestive heart failure. She denies having fever, chills, night sweats or weight loss. She has lived all her life in East Tennessee and has no history of exposure to tuberculosis. Three months prior, a tuberculin skin test was performed and showed a 0 mm induration. Her past medical history includes a fracture to one of her arms, also 3 months prior to the current visit. The medications she takes on a regular basis include aspirin, metoprolol, and furosemide. Her social history includes a 20 pack-year history of tobacco use, but quit for more than 25 years ago. She denies any alcohol consumption. ,
Physical Exam
On physical examination, patient was afebrile, pulse oximetry was 92% at 2 l/min of oxygen via nasal cannula, blood pressure was 125/80 mmHg, heart rate 85 beats per minute, respiratory rate 20 per minute. Pertinent positives on examination included a S3 on cardiac auscultation, lung auscultation was remarkable for diminished breath sounds, dullness at percussion and bibasilar crackles. The lower extremities revealed a 2 + pitting edema.
Lab
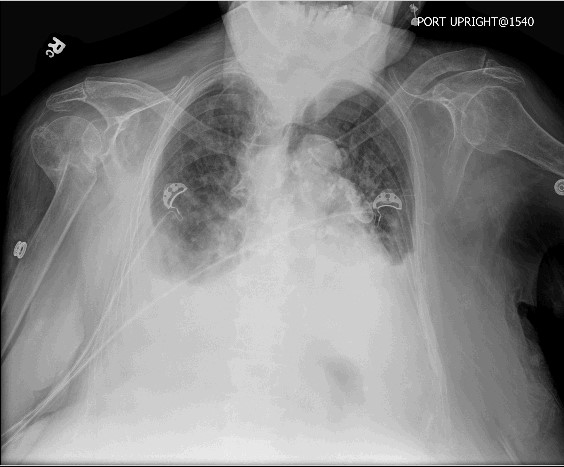
Laboratory analysis was only remarkable for a elevation of her creatinine to 1.8 mg/dL from a baseline value of1.3 mg/dL. The chest radiograph is shown below.
References
- Nissar Shaikh. Emergency management of fat embolism syndrome. J Emerg Trauma Shock. 2009 Jan-Apr; 2(1): 29–33.
- Strimlan CV, Dines DE, Payne WS. Mediastinal granuloma. Mayo Clin Proc. 1975 Dec;50(12):702-5.
- Parish J, Rosenow E. Mediastinal granuloma and mediastinal fibrosis. Semin Respir Crit Care Med 2002 Apr; 23(2):135-43
- Chan ED, Iseman MD. Potential association between calcified thoracic lymphadenopathy due to previous Histoplasma capsulatum infection and pulmonary Mycobacterium avium complex disease. South Med J 1999 Jun; 92(6):572-6
- Wheat LJ, Freifeld AG, Kleiman MB, et al. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007;45:807-825


