Reviewed By Allergy, Immunology & Inflammation Assembly
Submitted by
Luca Paoletti, MD
Fellow, Pulmonary/Critical Care Medicine
Division of Pulmonary and Critical Care Medicine
Medical University of South Carolina
Charleston, SC
P. Zachary Svigals, MD
P. Zachary Svigals, MD
Department of Internal Medicine
Medical University of South Carolina
Charleston, SC
J. Terrill Huggins, MD
Assistant Professor
Department of Medicine
Medical University of South Carolina
Charleston, SC
Nicholas J. Pastis, MD, FCCP
Assistant Professor
Department of Medicine
Medical University of South Carolina
Charleston, SC
Medical University of South Carolina
Medical University of South Carolina
Department of Medicine
Medical University of South Carolina
Charleston, SC
Submit your comments to the author(s).
History
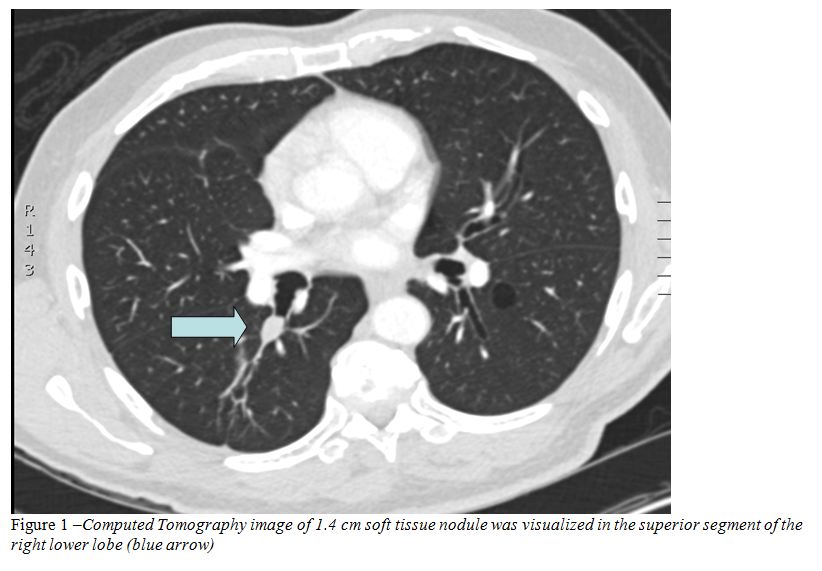
A 71 year old non-smoking African American man presented to an outpatient clinic for evaluation of an incidentally discovered lung nodule on a computed tomography (CT) scan of the chest. One week prior, the patient presented to the Emergency Department (ED) complaining of lightheadedness, generalized malaise, and dyspnea on exertion. He was able to walk approximately 50 yards until he had to rest to catch his breath. He also complained of a persistent dry non-productive cough, chronic rhinorrhea with white discharge, and a five pound unintentional weight loss over two months. The patient denied shortness of breath at rest, wheezing, hemoptysis, and chest pain. In the Emergency Department a computed tomography angiogram (CTA) of the chest was performed due to the suspicion of pulmonary embolus. While the CTA was negative for pulmonary embolus, a 1.4 cm soft tissue nodule was visualized in the superior segment of the right lower lobe (Figure 1) along with lower lobe bronchiectasis. The patient has had no prior imaging.
In the Emergency Department, he was diagnosed with a viral infection and volume depletion, he was given intravenous fluids and subsequently felt significantly better. Outpatient follow up was arranged for his lung nodule the following week.
His past medical history was significant for type 2 diabetes mellitus controlled with oral medications, gastroesophageal reflux disease, erectile dysfunction, and hypercholesterolemia. He denied prior surgeries. His medications included glucophage, glipizide, tadalafil and dexlansoprazole. He had no allergies and was a lifelong nonsmoker. His family history was unremarkable.
Physical Exam
Vital signs were within normal limits with an oxygen saturation of 100% on room air. Head and neck exam revealed no palpable lymphadenopathy or jugular venous distension. Lungs were resonant on percussion and clear to auscultation bilaterally. The cardiovascular exam revealed a regular rate and rhythm with normal S1 and S2 and no murmurs. The abdomen was soft and non-tender without hepatomegaly. Extremities revealed no clubbing, cyanosis or edema.
Lab
White blood count 8.5K/mm3, hemoglobin 12.0g/dL, hematocrit 37% platelet count of 220K/mm3. Sodium 134mmol/L, potassium 4.7mmol/L, chloride 102mmol/L, bicarbonate 22mmol/L, urea nitrogen 45mg/dL, creatinine 1.4mg/dL, calcium 9.1mg/dL. Brain Natriuretic Peptide (BNP) <10pg/mL.
Pulmonary function test two weeks prior showed an forced vital capacity (FVC) of 4.78L (118% of predicted), forced expiratory volume in 1 second (FEV1) of 3.92L (127% of predicted), FEV1/FVC ratio of 0.82, total lung capacity (TLC) of 6.91L (99% of predicted), residual volume (RV) of 2.0L (74% of predicted), and an unadjusted diffusing capacity of carbon monoxide (DLCO) of 18.2 (ml/min/mmHg) (82% of predicted).
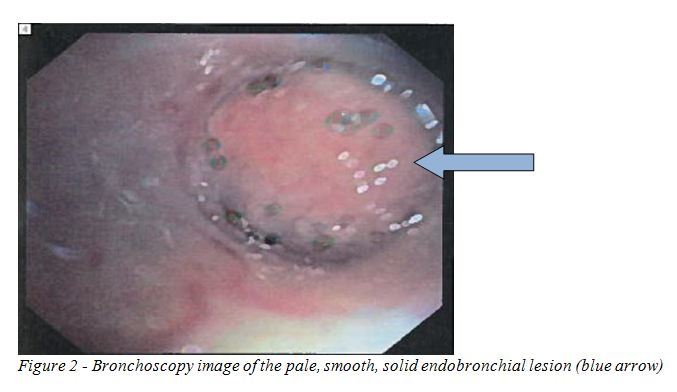
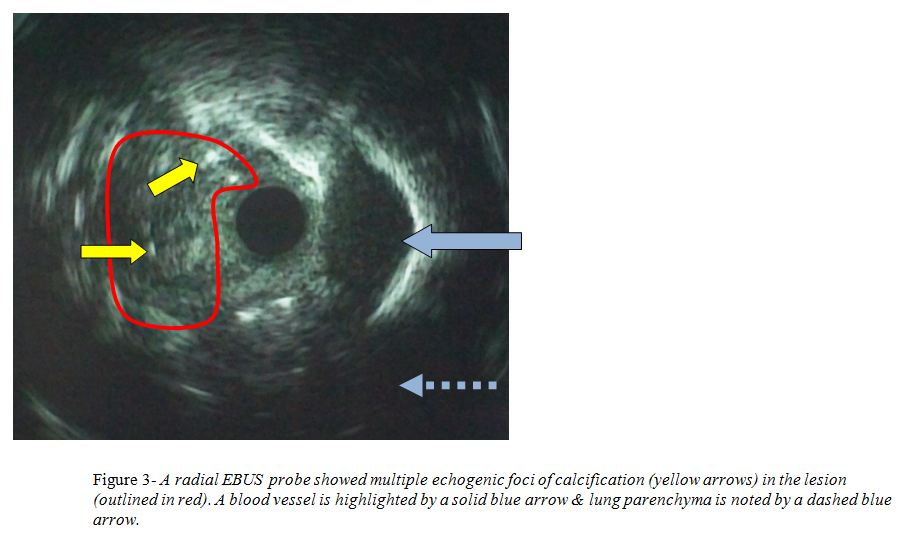
A flexible bronchoscopy was performed and a polypoid lesion was found occluding the orifice to the superior segment of the right lower lobe (Figure 2). A radial endobronchial ultrasound probe was used to further aid in the diagnosis of the lesion and it showed multiple echogenic foci of calcification (Figure 3). In order to diagnose the lesion and to restore patency of the airway an electrocautery snare was used to remove the lesion.
Figures
References
- Gomez M, Silvestri GA. Endobronchial ultrasound for the diagnosis and staging of lung cancer. Proc Am Thorac Soc 2009;6:180-6.
- Yasufuku K, Nakajima T, Chiyo M, Sckine Y, Shibuya K, Fujisawa T. Endobronchial ultrasonography: current status & future directions. J Thorac Oncol 2007;10:970-9.
- Wang Memoli JS, Nietert PJ, Silvestri GA. Meta-Analysis of guided bronchoscopy for the evaluation of the pulmonary nodule. Chest [Epub ahead of print] 2011 Oct 6 [cited 2012 March 12]. Available from: http://chestjournal.chestpubs.org/content/early/2011/10/04/chest.11-1764.
- Gjevre JA, Myers JL, Prakash UB. Pulmonary hamartomas. Mayo Clin Proc 1996;71:14-20.
- Albrecht E. Ueber hamartome. Verh Dtsch Ges Pathol 1904;7:153-157.
- Ost D, Fein AM, Feinsilver SH. Clinical practice. The solitary pulmonary nodule. N Engl J Med 2003;348:2535-42.
- Cosío BG, Villena V, Echave-Sustaeta J, de Miguel E, Alfaro J, Hernandez L, Sotelo T. Endobronchial hamartoma. Chest 2002;122:202-5.
- Fletcher JA, Pinkus GS, Donovan K, Naeem R, Sugarbaker DJ, Mentzer S, Pinkus JL, Longtine J. Clonal rearrangement of chromosome band 6p21 in the mesenchymal component of pulmonary chondroid hamartoma. Cancer Res 1992;52:6224-8.
- Johansson M, Dietrich C, Mandahl N, Hambraeus G, Johansson L, Clausen PP, Mitelman F, Heim S. Recombinations of chromosomal bands 6p21 and 14q24 characterise pulmonary hamartomas. Br J Cancer 1993;67:1236-41.
- Wilson RW, Kirejczyk W. Pathological and radiological correlation of endobronchial neoplasms: Part I, Benign tumors. Ann Diagn Pathol 1997;1:31-46.
- Murray J, Kielkowski D, Leiman G. The prevalence and age distribution of peripheral pulmonary hamartomas in adult males. An autopsy-based study. S Afr Med J 1991;79:247-9.
- McDonald JR, Harrington SW, Clagett OT. Hamartoma (often called chondroma) of the lung. J Thorac Surg 1945; 14:128-143.
- Tomashefski Jr J. Benign endobronchial mesenchymal tumors. Their relationship to parenchymal pulmonary hamartomas. Am J Surg Pathol 1982; 6:531-540.
- Borro J, Moya J, Botella J, Padilla J, Canto A, Paris F. Endobronchial hamartoma. Report of 7 cases. Scand J Thor Cardiovasc Surg 1989; 23:285-287.
- Van den Bosch J, Wagenaar S, Corrin B, Elbers J. Mesenchymoma of the lung (so-called hamartoma): a review of 154 parenchymal and endobronchial cases. Thorax 1987; 42:790-793.
- Hansen C, Holtveg H, Francis D, Rasch L, Bertelsen S. Pulmonary hamartoma. J Thorac Cardiovasc Surg 1992; 104:674-678.
- Fudge T, Ochsner J, Mills N. Clinical spectrum of pulmonary hamartomas. Ann Thorac Surg 1980; 30:36-39.
- Bateson E. So-called hamartoma of the lung--a true neoplasm of fibrous connective tissue of the bronchi. Cancer 1973; 31:1458-1467.
- Sibala JL. Endobronchial hamartomas. Chest 1972;62:631-4.
- Siegelman SS, Khouri NF, Scott WW Jr, Leo FP, Hamper UM, Fishman EK, Zerhouni EA. Pulmonary hamartoma: CT findings. Radiology 1986;160:313-7.
- Good CA, Wilson TW. The solitary circumscribed pulmonary nodule. JAMA 1958;166:210-215.
- Park CM, Goo JM. Images in clinical medicine. "Popcorn" calcifications in a pulmonary chondroid hamartoma. N Engl J Med 2009;360:e17.
- Good CA. Management of patient with solitary mass in lung. Chic Med Soc Bull 1953;55:893-896.
- Khan AN, Ghanem SA, Irion KL, MacDonald S, Allen CM. Lung Hamartoma Imaging. Medscape 2011 May 27 [cited 2011 Feb 28]. Available from: http://emedicine.medscape.com/article/356271-overview.
- Huang Y, Xu D, Jirapatnakul A, Reeves AP, Farooqi A, Zhang L, Giunta S, Zulueta J, Aye R, Miller A, Mendelson DS, Aylesworth C, Sheppard B, Klingler K, Yankelevitz DF, Henschke CI. CT- and computer-based features of small hamartomas. Clin Imaging 2011;35:116-22.
- Ledor K, Fish B, Chaise L, Ledor S. CT diagnosis of pulmonary hamartomas. J Comput Tomogr 1981;5:343-4.
- Guo W, Zhao YP, Jiang YG, Wang RW, Ma Z. Surgical treatment and outcome of pulmonary hamartoma: a retrospective study of 20-year experience. J Exp Clin Cancer Res 2008;27:8.
- Park KY, Kim SJ, Noh TW, Cho SH, Lee DY, Paik HC, Ryu YH. Diagnostic efficacy and characteristic feature of MRI in pulmonary hamartoma: comparison with CT, specimen MRI, and pathology. J Comput Assist Tomogr 2008;32:919-25.
- Herth F, Ernst A, Schulz M, Becker H. Endobronchial ultrasound reliably differentiates between airway infiltration and compression by tumor. Chest 2003;123:458-62.
- Wang Memoli JS, El-Bayoumi E, Pastis NJ, Tanner NT, Gomez M, Huggins JT, Onicescu G, Garrett-Mayer E, Armeson K, Taylor KK, Silvestri GA. Using EBUS Features to Predict Lymph Node Metastasis in Patients with Lung Cancer. Chest 2011;140:1550-6.
- Fujiwara T, Yasufuku K, Nakajima T, Chiyo M, Yoshida S, Suzuki M, Shibuya K, Hiroshima K, Nakatani Y, Yoshino I. The utility of sonographic features during endobronchial ultrasound-guided transbronchial needle aspiration for lymph node staging in patients with lung cancer: a standard endobronchial ultrasound image classification system. Chest 2010;138:641-7.
- Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom RM, Gareen IF, Gatsonis C, Marcus PM, Sicks JD. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011;365:395-409.


