An unexpected etiology of ventricular dysrhythmia
Megan Acho, MD
Fellow, Division of Pulmonary, Allergy, and Critical Care Medicine, University of Pittsburgh Ian Barbash, MD, MS
Assistant Professor, Division of Pulmonary, Allergy, and Critical Care Medicine, University of Pittsburgh
Case
A 41-year-old man with a history of alcohol and cocaine abuse presented to the emergency department after experiencing an out-of-hospital cardiac arrest while at a party. Cardiopulmonary resuscitation was administered by bystanders and return of spontaneous circulation was achieved. He was intubated in the field. On arrival to the emergency room, he was bradycardic with a heart rate of 36, PR interval of 214 milliseconds, QRS of 148 milliseconds, and a corrected QT interval of 600 milliseconds. Vital signs were also noteworthy for hypotension to the 90s/30s mmHg. Urine toxicology was negative for cocaine and tricyclic antidepressants. He was admitted to the Medical Intensive Care Unit.
The patient was started on dopamine, norepinephrine, and isoproterenol infusions. Electrocardiography demonstrated a PR interval of 68 milliseconds, QRS of 186 milliseconds and a corrected QT interval of 641 milliseconds with the following rhythm:
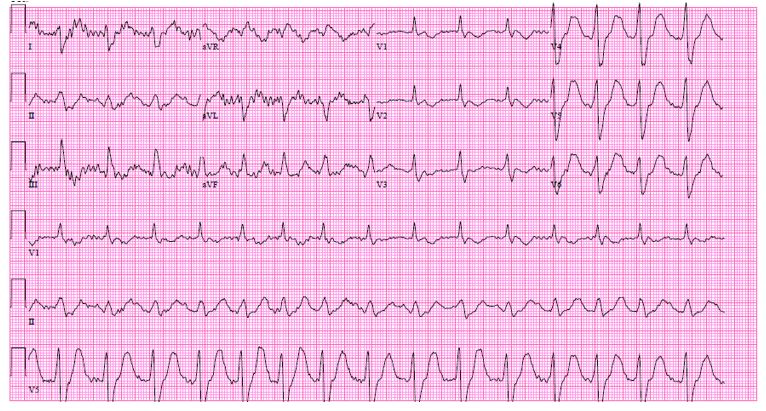
His rhythm subsequently degenerated into ventricular tachycardia.
Question
1) An excessive dose of which of the following is the most likely etiology of this patient's abnormal electrocardiographic findings?
- Cocaine
- Loperamide
- Metoprolol
- Midazolam
- Nortriptyline
2) In addition to initiating Advanced Cardiac Life Support (ACLS) protocol, which of the following is the best treatment at this time?
- Administer intravenous flecainide
- Initiate transvenous pacing
- Administer intravenous sodium bicarbonate
- Administer intravenous beta blockade
Answers:
1) B. Loperamide
2) C. Administer intravenous sodium bicarbonate
Discussion
The electrocardiographic findings of QT prolongation and progressive QRS widening were attributed to loperamide toxicity. Regarding Question 1, though cocaine and nortriptyline may also potentiate QT prolongation and ventricular dysrhythmias, the patient's urine toxicology was negative for both drugs. Metoprolol and midazolam do not cause QT prolongation or ventricular arrhythmias and, as such, are incorrect answer choices. Further discussion with the patient's friends and family revealed that he had been taking approximately 200 2-milligram tablets of loperamide daily in the weeks preceding this presentation. Loperamide is an opioid agonist available over-the-counter as an antidiarrheal agent. The drug slows intestinal motility by acting on opiate receptors within the gut; at appropriate dosing it has low bioavailability, poor penetration of the blood-brain-barrier, and a minimal side effect profile. At higher concentrations, loperamide can cause respiratory depression and arrhythmias. Loperamide blocks potassium channels, resulting in significant QT prolongation and torsades de pointes. At even higher plasma concentrations, loperamide causes sodium channel blockade, resulting in QRS complex widening.
Treatment of loperamide toxicity is focused on maintaining cardiopulmonary stability. If patients present within several hours of ingestion, gastric decontamination may minimize systemic absorption, although in many cases the highest plasma concentrations result from chronic ingestion. Opioid antagonists may mitigate respiratory depression, though some patients will require intubation and mechanical ventilation. Aggressive medical management of cardiac toxicity is required to prevent and treat arrhythmias. Electrolyte supplementation should be provided to ensure that the patient's potassium is greater than 4 millimoles per liter and the magnesium is greater than 2 milligrams per deciliter. When significant widening of the QRS complex is noted (as seen on this electrocardiogram), intravenous sodium bicarbonate should be administered to narrow the QRS complex (Question 2). In cases of severe arrhythmias complicated by hemodynamic compromise that are refractory to initial medical management, placement of a transvenous pacer should be considered for overdrive pacing. Flecainide, a class Ic antiarrhythmic, would cause increased sodium channel blockade with QRS complex widening and, as such, is not appropriate. Beta blockade is also inappropriate, as this would exacerbate the patient's bradycardia.
In cases of bradycardia associated with ventricular ectopy, isoproterenol is typically used, though intravenous infusions can be complicated by vasodilation and worsening hemodynamics. Lidocaine may reduce the burden of ventricular ectopy. Amiodarone may worsen QT prolongation and paradoxically exacerbate arrhythmias. If pulseless ventricular tachycardia or ventricular fibrillation occurs, providers should follow ACLS protocol. Case studies support a potential benefit from intravenous lipid emulsions and veno-arterial extracorporeal membrane oxygenation in refractory cases.
In the context of today's devastating opioid epidemic, loperamide has garnered increasing attention for its ability to potentiate a "high" and to mitigate symptoms of opioid withdrawal when used in excess. The recommended dose is 2-4 milligrams in adults, not to exceed 16 milligrams daily. As a non-prescription drug, loperamide can be purchased in bulk, with many retailers selling up to 200 capsules at a time for about $25.00. Cardiotoxicity has most often been seen in chronic overuse of loperamide. In 2016, the Food and Drug Administration issued a Drug Safety Communication to warn about "serious heart problems that can lead to death" associated with inappropriate loperamide use. Anecdotally, our own intensive care unit has seen a handful of cases of ventricular arrhythmias due to loperamide over the past year and, nationally, these numbers are on the rise. Intensivists should familiarize themselves with the complications of loperamide misuse and the ways in which to manage these patients.
References:
-
FDA Drug Safety Communication: FDA warns about serious heart problems with high doses of the antidiarrheal medicine loperamide (Imodium) including from abuse and misuse. Food and Drug Administration, June 2016. (https://www.fda.gov/downloads/Drugs/DrugSafety/UCM505108.pdf).
-
Litovitz T, Clancy C, Korberly B, et. al. Surveillance of loperamide ingestions: an analysis of 216 poison center reports. J Toxicol Clin Toxicol 1997; 35: 11-9.
-
MacDonald R, Heiner J, Villarreal J, et. al. Loperamide dependence and abuse. BMJ Case Reports 2015. doi:10.1136/bcr-2015-209705
-
Miller H, Panahi L, Tapia D, et. al. Loperamide misuse and abuse. Journal of the American Pharmacists Association 2017; 57: S45-S50.
-
Wu PE, Juurlink DN. Clinical Review: Loperamide Toxicity. Annals of Emergency Medicine 2017; 70: 245-52.


