Cheyne-Stokes Respiration
Aaron Roberts, MD; Ninotchka L. Sigua, MD
Case
46 year old male was sent by his primary care physician for a sleep study for symptoms of daytime fatigue and poor sleep. In addition, he snores and wakes up gasping for air during sleep. Medical history is significant for hypertension, diabetes mellitus and dilated cardiomyopathy with an ejection fraction of 20%. Medications include carvedilol, furosemide, pravastatin, lisinopril, hydralazine and isosorbide mononitrate.
His baseline polysomnogram is shown below.
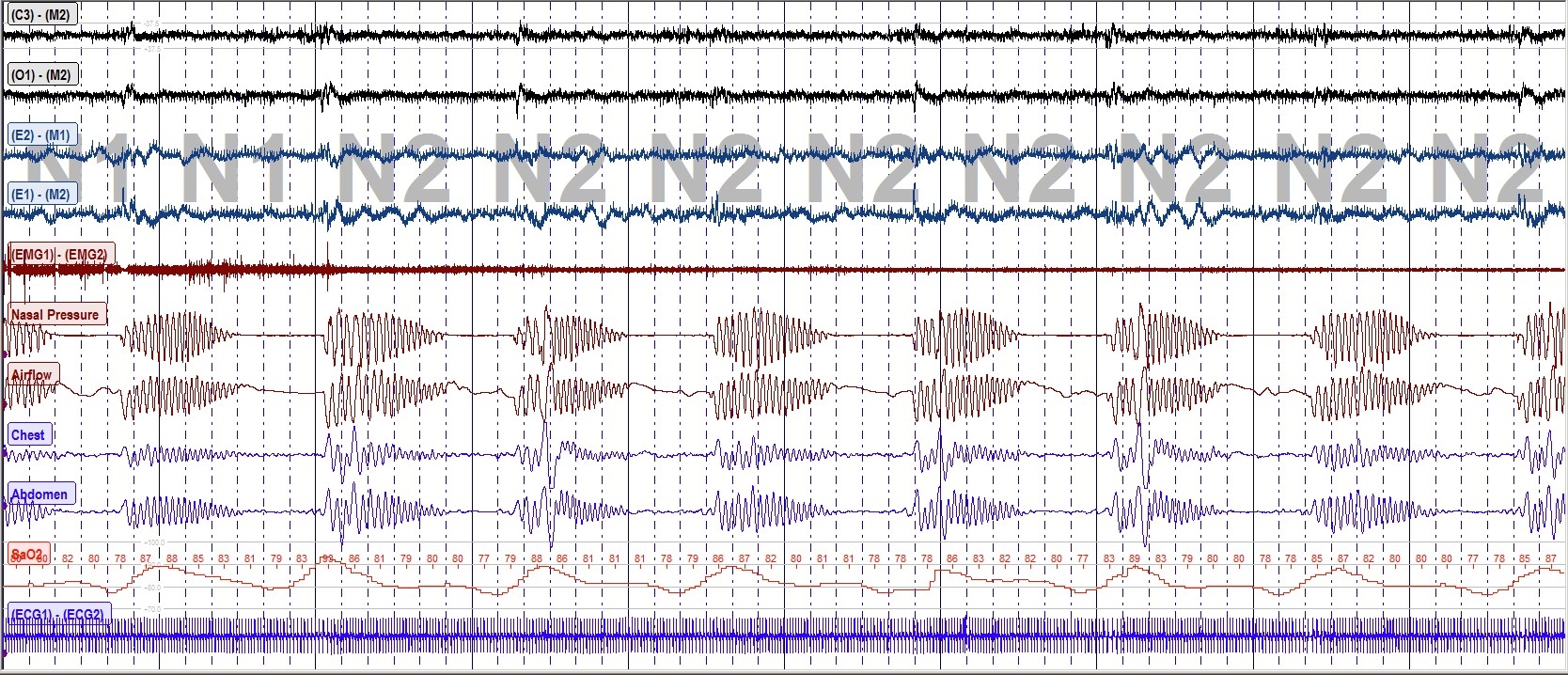
What is the diagnosis?
- Obstructive Sleep Apnea
- Cheyne Stokes Respiration
- Primary Central Sleep Apnea
- Sleep-related Hypoxemia
Answer: b) Cheyne-Stokes Respiration (CSR)
Cheyne-Stokes respiration (CSR) is characterized by the cessation of airflow and respiratory effort alternating with periods of hyperventilation. This crescendo-decrescendo breathing pattern can be seen during wake and sleep and when it occurs during sleep is part of central sleep apnea syndrome. A typical cycle lasts for about 45 to 90 seconds and is primarily seen during non–rapid eye movement (NREM) sleep stages 1 and 2. Epidemiologic studies have shown an estimated prevalence of 40% of CSR and central sleep apnea in patients with systolic heart failure. Additional risk factors include symptomatic heart failure with preserved ejection fraction (diastolic dysfunction), male gender, advanced age, atrial fibrillation, nocturnal ventricular arrhythmias, low arterial partial pressure of CO2 (Paco2), reduced exercise capacity and very low ejection fraction (<20%). It has also been reported in patients with neurologic disorders, renal failure and those who ascend rapidly to high altitudes. CSR results from ventilatory control instability (high loop gain) due to increased chemosensitivity and circulatory delay resulting to a cyclical pattern of hypocapnia, hypercapnia and hypoxia. Management of CSR should focus on the underlying mechanisms by which CHF increases loop gain and promotes unstable breathing. Current treatment strategies include optimization of heart failure, CPAP therapy, oxygen supplementation, ASV in selected patients and respiratory stimulants.
References:
-
Javaheri S, Parker TJ, Liming JD, Corbett WS, Nishiyama H, Wexler L, Roselle GA. Sleep apnea in 81 ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations. Circulation 1998;97(21):2154-9.
-
Sands SA, Owens RL. Congestive heart failure and central sleep apnea. Crit Care Clin. 2015 Jul;31(3):473-95. doi: 10.1016/j.ccc.2015.03.005.


