"The Breathing Dead"
Burton W. Lee, MD
Pulmonary Critical Care Section
Medstar Washington Hospital Center
Associate Professor of Medicine
Georgetown University School of Medicine
Consider a patient with massive intracerebral hemorrhage on volume cycled AC mode as follows: 30% FIO2 / Vt 0.5 L / rate 12 / PEEP 5 / flow 55 lpm decelerating pattern / flow triggering 2 lpm. Patient has fixed dilated pupils, exhibits no brainstem reflexes and is unresponsive to all stimuli. However, it appears she is breathing at a rate of 20 when the set ventilator rate is 12. Therefore an apnea test is being deferred. Below are the pressure-time (top) and flow-time (bottom) curves for the patient. What is happening to this patient?
A. Delayed Expiratory Cycling - Prolonged inspiration due to an inappropriately low inspiratory flow setting.
B. Inspiratory Flow Starvation.
C. Ineffective Triggering
D. Autotriggering

Correct answer is D.
When the sensitivity setting is switched from flow (sensitivity of 2 lpm) to pressure triggering (sensitivity of 2 cm H2O), patient no longer breathes above the ventilator. The pressure-time (top) and flow-time (bottom) curves for both sensitivity settings are shown below.

Flow Triggering
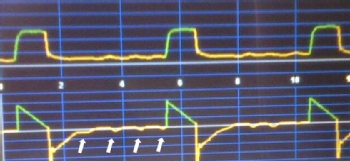
Pressure Triggering
Why does the patient’s respiratory rate decrease with pressure triggering? Recall that flow triggering is generally more sensitive than pressure triggering. This patient was actually brain dead and made no respiratory effort but the ventilator was being triggered by the patient’s heartbeat (arrowhead). This is known as autotriggering or autocycling. Autotriggering may occur whenever an artifact (e.g. heartbeat, secretions, endotracheal cuff leak or bronchopleural fistula) leads to unintended triggering of the ventilator. When the ventilator is switched to a less sensitive but still reasonable trigger threshold (e.g. pressure of 2 cm H2O), the ventilator is no longer falsely triggered by the heartbeats (arrows). Alternatively, a less sensitive flow trigger threshold would have also had the same effect. Therefore, the patient’s flow triggering setting was overly sensitive for this situation and was in fact masking brain death.


