My Neck Hurts and I Can’t Breathe
Alexandra Levine DO
Resident Physician, Department of Medicine, Morristown Medical Center, Morristown, NJ
Case
A 30-year-old female with a history of type 1 diabetes, IV drug use and attention deficit hyperactivity disorder presented to the emergency department after her family found her unresponsive at home. She was treated with narcan in the field for which the patient subsequently became more awake and responsive. Upon arrival to the hospital she was found to be hypotensive to the 70-80s/40s, hypothermic and tachycardic. Physical exam was remarkable for upper and lower extremity edema, scabbed lesions on her right foot and ankle, and a 5 cm area of erythema and induration at the base of her neck, with a central area of fluctuance and skin necrosis suggestive of an abscess. She was admitted to the intensive care unit and over the course of the following day her respiratory status worsened for which she was intubated. Labs were significant for MRSA bacteremia as well as MRSA growing in cultures drawn from her neck abscess upon drainage.
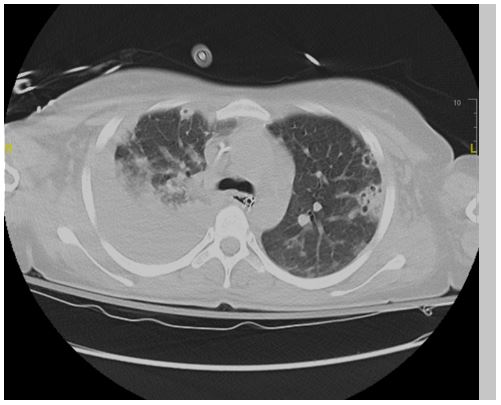
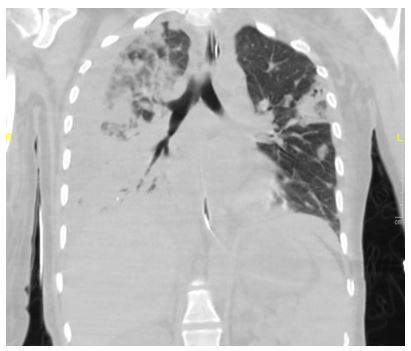
A high-resolution CT chest was obtained:
Question
What is the likely etiology of her findings on CT imaging?
- Pulmonary Embolism
- Septic Emboli
- Granulomatosis with Polyangitis
- Foreign Body Granulomatosis
- Malignancy
B. Septic emboli, likely due to her IV drug use
Discussion
The patient was found to have multifocal cavitary pneumonia secondary to septic emboli, likely in the setting of her IV drug use, neck abscess and MRSA bacteremia. Septic pulmonary embolism is a fairly uncommon disorder in which an infected thrombus causes a mechanical obstruction in the pulmonary vasculature. Patients can present with signs and symptoms ranging in severity from dyspnea, cough, chest pain, and fevers to hemoptysis or septic shock. Patients are diagnosed by characteristic findings on CT scan coupled with a source of infection. Our patient’s CT scan demonstrates several features of septic emboli and its complications, including:
- Bilateral peripheral, nodular lesions in various stages of cavitation
- Parapneumonic effusions, which can progress to empyema
- Feeding vessel signs (a branch of a pulmonary artery leading directly to a nodule or mass)
- A possible subpleural wedge-shaped density in the left lung concerning for pulmonary infarct
Identifying a microbial pathogen in the blood, sputum, soft tissue (if indicated), or implanted device is important for guiding therapy. High risk individuals include IV drug users, immunocompromised patients, patients with indwelling devices including pacemaker wires, central venous catheters or other prosthetics, as well as those with periodontal disease or documented infection elsewhere in the body. Septic pulmonary emboli are most common among patients with right sided endocarditis, and can be seen in up to 75% of patients with tricuspid vegetations. Staph aureus is the most common pathogen isolated and includes both methicillin-sensitive disease and MRSA. Our patient was an IV drug user which is likely the origin of her bacteremia and abscess formation. An initial transthoracic echocardiogram performed did not reveal any valvular vegetations or disease; However ultimately a TEE performed in the subsequent days revealed a 1.0 x 1.3 cm vegetation on the tricuspid valve. In addition to endocarditis with valvular vegetations, an extrathoracic site of infection can cause bacterial translocation into the systemic circulation, producing direct or indirect damage via released toxins and inflammatory mediators. These mediators promote local thrombosis, which can create additional sites of bacterial proliferation that may ultimately embolize to the pulmonary vasculature.
Early treatment is crucial and includes antimicrobial therapy and possibly invasive procedures directed toward source control. If treatment is delayed, complications can include pulmonary infarcts, pulmonary abscesses, pleural effusions, empyema and pneumothorax. Antimicrobial treatment duration is for a minimum of 4-6 weeks, during which patients are assessed for clinical improvement and blood cultures are re-tested to confirm clearance. Ultimately the patient expired about one week from presentation due to complications including pulmonary abscess formation, empyema formation, kidney failure, septic and cardiogenic shock.
References
-
Brenes, Jorge A. “The Association of Septic Thrombophlebitis with Septic Pulmonary Embolism in Adults.” The Open Respiratory Medicine Journal, vol. 6, no. 1, 2012, pp. 14–19., doi:10.2174/1874306401206010014.
-
Goswami, Umesh, et al. “Associations and Outcomes of Septic Pulmonary Embolism.” The Open Respiratory Medicine Journal, vol. 8, no. 1, 2014, pp. 28–33., doi:10.2174/1874306401408010028.
-
Iwasaki, Yoshinobu, et al. “Spiral CT Findings in Septic Pulmonary Emboli.” European Journal of Radiology, vol. 37, no. 3, 2001, pp. 190–194., doi:10.1016/s0720-048x(00)00254-0.
-
Singh, Jatinder, et al. “Clinical Course Of Patients With Septic Pulmonary Embolism Among Injection Drug Users With Infective Endocarditis.” Chest, vol. 132, no. 4, 2007, doi:10.1378/chest.132.4_meetingabstracts.501a.


