Pulsus Paradoxus in High Risk PE on Positive Pressure Ventilation
Megan Conroy, MD 1, Jerry Ash, MD2, Edwin Jackson Jr, DO1
1. Division of Pulmonary, Critical Care, and Sleep Medicine, The Ohio State University Wexner Medical Center
2. Department of Internal Medicine, The Ohio State University Wexner Medical Center
A 48-year-old female is transferred to the MICU with hypoxic respiratory failure and shock. The patient is intubated and placed on positive pressure ventilation with settings AC/VC, Vt 390, RR 22, PEEP 8, FiO2 100%, vasopressors are administered and radial arterial line is placed.
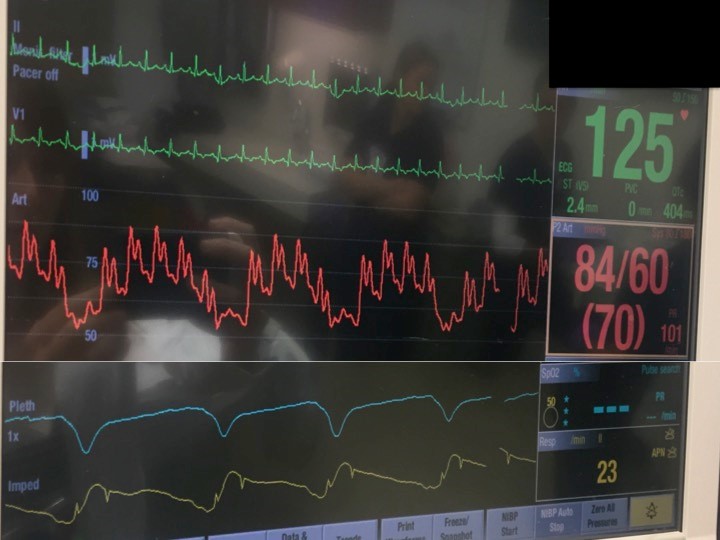
Upon insertion the arterial line shows the following waveform:
Question
Arterial line waveform exhibits which of the following:
- Pulsus parvus et tardus
- Pulsus paradoxus
- Pulsus alternans
- Overdampening
Pulses paradoxus
Discussion
The arterial waveform exhibits a significant reduction in systolic blood pressure with inspiration, a finding known as pulsus paradoxus.
Findings of pulsus paradoxus on arterial line waveform should prompt rapid assessment of potential causes, which may include cardiac tamponade, pulmonary embolism, severe acute asthma, exacerbations of chronic obstructive pulmonary disease, and pericardial disease1.
Pulsus parvus et tardus refers to the slow upstroke and small amplitude of palpated pulse which can be seen in aortic stenosis. Pulsus alternans describes a pattern of varying amplitude from one beat to the next, reflecting a beat-to-beat variation in cardiac output.
The dampening coefficient of a pressure monitoring system will impact the exaggeration or elimination of low- or high-frequency components of the complex wave-form. An overdampened system smoothes the tracing and will underestimate systolic pressure. An underdampened system will exaggerate some components of the waveform and overestimate systolic pressure2.
In the case presented here, bedside cardiac ultrasonography was performed and showed the following image consistent with RV pressure-volume overload (dilatation of the right ventricle with high RV/LV ratio, abnormal leftward bowing of the interventricular septum, RV basal and mid free wall hypokinesis with sparing of the apex, known as McConnell's sign)
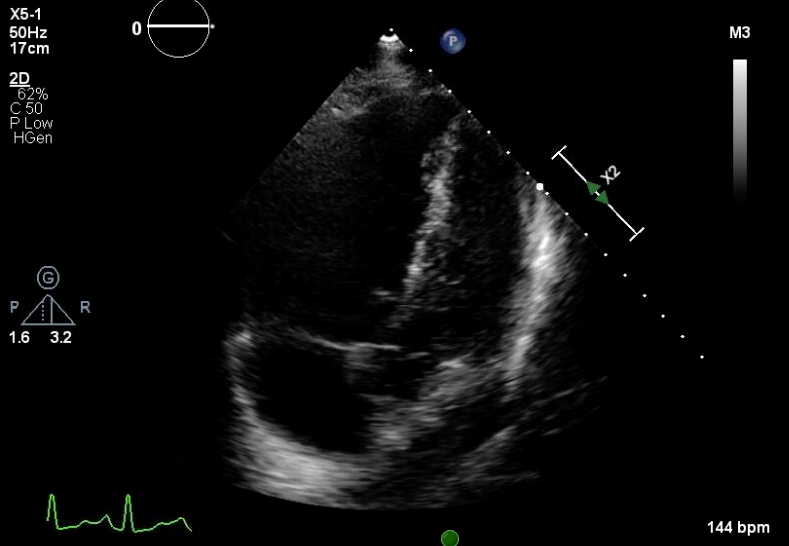
Echocardigraphy is further notable for a lack of pericardial effusion. Bedside lower extremity ultrasound was notable for non-compressible left femoral vein, consistent with deep venous thrombosis. Findings were most consistent with a massive (high risk) pulmonary embolism in the setting of persistent systemic hypotension. Given these bedside echocardiographic findings, the patient was treated with systemic thrombolytic therapy, but unfortunately died within 12 hours. Post mortem examination was performed, and confirmed the diagnosis of pulmonary embolism.
When a patient is mechanically ventilated with positive pressure, systolic blood pressure is typically higher during inspiration than expiration, termed reversed pulsus paradoxus, due to decreased left ventricular afterload3.
However, this patient's arterial line waveform exhibits a significant reduction in systolic blood pressure during inspiration on positive pressure ventilation due to parallel biventricular interdependence and transmission of positive intrathoracic pressure across a dilated RV resulting in leftward shift of interventricular septum and reduction in LV filling.
References
-
Hamzaoui O, Monnet X, Teboul JL. Pulsus Paradoxus. European Respiratory Journal 2013. 42:1696-1705
-
Leatherman JW, Marini J. Chapter 28: Interpretation of Hemodynamic Waveforms. In: Hall JB, Schmidt GA, Kress JP. Principles of Critical Care. 4th ed. ;McGraw-Hill; 2015
-
Abel JG, Salerno TA, Panos A, Greyson ND, Rice TW, Teoh K, Lichtenstein SV. Cardiovascular effects of positive pressure ventilation in humans. Ann Thorac Surg. 1987 Feb; 42(2):198-206.


