Shortness of Breath After Vertebroplasty
Michelle Bernshteyn, Alyssa Cortese, Amitpal Nat
SUNY Upstate Medical University
Case
A 76-year-old female patient with a past medical history of osteoporosis, seizure disorder, and hypertension who presented to the hospital after an unwitnessed fall and seizure-like activity. The patient was found to have an unstable 3-column L1 ankylosed spine fracture and Neurosurgery was consulted. The patient underwent vertebroplasty, T9-pelvis decompression and fusion with cement augmentation. Over the course of the day following surgery, the patient experienced increased work of breathing. This was evidenced by elevated respiratory rate and oxygen desaturation requiring oxygen supplementation via nasal cannula. On physical examination, she was noted to have diminished breath sounds on auscultation of the right lower lobe.
Images
Question
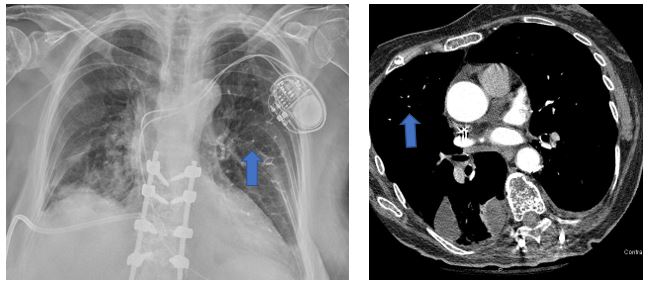
What is the finding as pointed out by blue arrows?
- Cement Emboli
- Pulmonary Nodules
- Pneumonia
- Pulmonary Emboli
Answer: A. Cement Emboli
Discussion
Cement emboli are seen in these imaging modalities, as pointed out by the blue arrows. These radiopaque densities involve the distal pulmonary arteries and is related to the patient’s recent vertebroplasty. Vertebroplasties are performed to restore height, stabilize bony trabeculae, and alleviate pain. During a vertebroplasty, polymethyl methacrylate (a cement compound) is introduced into the vertebral body. Rarely, it extravasates into the vertebral venous plexus and migrates into the IVC and pulmonary arterial system. Based on literature review, 0.4-0.9% of patients who undergo vertebroplasties are found to have cement emboli. This can present as dyspnea, tachycardia, and/or tachypnea. Even though there have been a limited number of cases involving this complication, onset of symptoms ranged from ages 15 to 96 and involved approximately 65% females and 35% males. Many times patients present with acute onset dyspnea and chest pain. Risk factors were not identified.
Cement emboli can be diagnosed with plain films. On CT scan, cement emboli are differentiated from thrombi by diameter, length, caliber, and radio-opacity. Based on limited case reports, it is thought that the treatment of cement emboli should include anticoagulation. Warfarin or enoxaparin for approximately three months can be used and helps prevent thrombosis around the cement.
References:
-
Rahimi B, Boroofeh B, Dinparastisaleh R, et. al. Cement pulmonary embolism after percutaneous vertebroplasty in a patient with cushing's syndrome: A case report. Respir Med Case Rep 2018; 25: 78–85.
-
Oshinsky C, Bhavani S, Funaki A. Cement cardiac embolism following kyphoplasty noted on thoracic imaging. Radiol Case Rep 2018; 13(4): 914–6.
-
Siddiqui AS, Goodarzi A, Majumdar T, et. al. A rare case of pulmonary cement embolism in a lung transplant patient. Respir Med Case Rep 2018; 24: 63–4.
-
Bernhard J, Heini PF, Villiger PM. Asymptomatic diffuse pulmonary embolism caused by acrylic cement: an unusual complication of percutaneous vertebroplasty. Ann Rheum Dis 2003; 62(1):85–6.
-
Duijvelshoff R, Anthonissen NFM, Morshuis WJ, et. al. Intracardiac cement embolism resulting in tricuspid regurgitation. European Journal of Cardio-Thoracic Surgery 2019; 55(2): 366–8.


