Shortness of Breath with History of Cardiac Arrest
SUNY Upstate Medical University
Case:
A 64-year-old male with a past medical history significant for chronic obstructive pulmonary disease, diastolic congestive heart failure, obstructive sleep apnea, and history of cardiac arrest three years prior requiring CPR, presented to the hospital due to shortness of breath. His vital signs on presentation were as follows: blood pressure 120/80 mmHg, heart rate 105 beats per minute, body temperature 37C, respiratory rate of 22 breaths per minute, and oxygen saturation of 89% on room air. His physical examination demonstrated diminished breath sounds diffusely. His clinical presentation and chest x-ray were compatible with pneumonia. This was the patient’s first episode of pneumonia. The patient was subsequently intubated and computed tomography (CT) scan was then performed due to his worsening respiratory status.
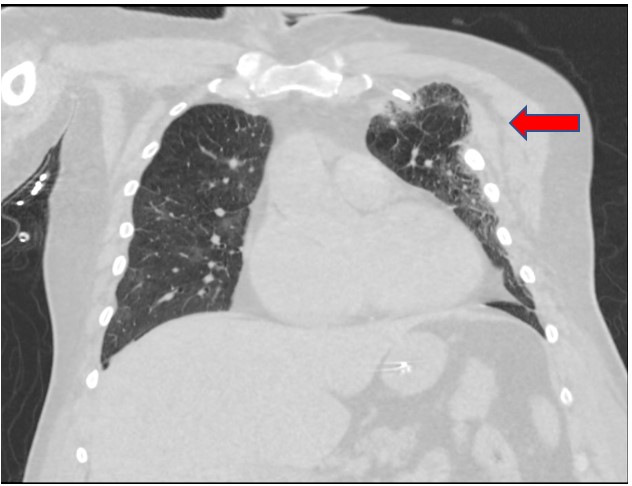
Figure 1
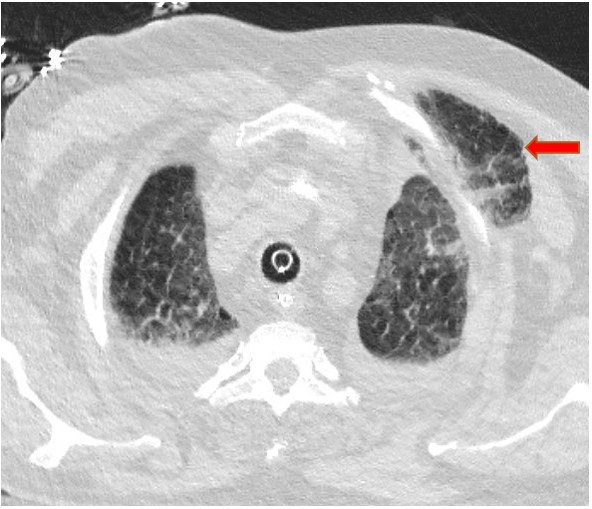
Figure 2
Question:
What is the finding as pointed out by the red arrows?
- Teratoma
- Necrotizing fasciitis
- Chest wall abscess
- Herniated lung
D. Herniated lung
Discussion:
This CT scan demonstrates an extra-thoracic herniation of the left lung (answer choice D). Lung tissue can be visualized anterior to the ribs as pointed out by the red arrow.
Teratoma (answer choice A) is incorrect as this would usually appear in the mediastinum and may contain variable imaging features such as a well-demarcated shape, evidence of fat, and calcifications. Necrotizing fasciitis (answer choice B) is incorrect as this would involve gas within fluid collections, as well as fat stranding. Finally, chest wall abscess (answer choice C) is incorrect as abscesses tend to have a well-defined capsule with inflammatory changes. The patient did not demonstrate signs of active infection.
The patient sustained multiple rib fractures during resuscitative efforts when he suffered a cardiac arrest three years ago. The herniation of his left lung was an incidental finding on CT imaging. Treatment of herniated lungs can include approximation of the ribs. The patient’s presentation of dyspnea was not attributed to this finding; thus, treatment was not pursued. His dyspnea was attributed to pneumonia and he was treated with antibiotics.
A herniated lung is not a common finding. In one study performed in 1968, only 260 cases had been reported globally [1]. It is most commonly acquired from trauma to the chest or after operative procedures with inadequate chest wall closure [2]. Herniation of the lung can also be a spontaneous process. When it does occur spontaneously, the patient usually has a history of chronic obstructive pulmonary disease or prolonged steroid use [1]. Sometimes it is precipitated by a cough, sneeze, or other process that abruptly increases intrathoracic pressure [3].
Herniated lung can present immediately after these events or can be delayed by several years. It often presents as localized pleuritic chest pain, dyspnea, and cough that does not respond to conservative therapy [3]. Physical examination findings may include a chest wall defect or mass [1]. The Valsalva maneuver can cause the lung to bulge from the chest and become more visible, aiding in diagnosis [2].
Asymptomatic lung hernias are usually treated conservatively, but when symptomatic they can be surgically treated [1]. Complications such as pleural scarring, recurrent pneumonia, and pneumonitis can occur and would be indications for surgical intervention [1]. Fortunately, this was the patient’s first episode of pneumonia and therefore he did not meet the indications for surgical intervention.
References
-
Cox M, Thota D, Trevino R, “Spontaneous Lung Herniation Through the Chest Wall” Military Medicine, vol. 183, issue 3-4, pp. 233-234, 2018. https://doi.org/10.1093/milmed/usx063.
-
Weissberg D, Refaely Y, “Hernia of the lung” Ann Thorac Surg, vol. 74, no. 6, pp. 1963-1966, 2002. doi: 10.1002/rcr2.354.
-
Hamid M, et al. “Spontaneous Lung Herniation Leading to Extensive Subcutaneous Emphysema, Pneumothorax, Pneumomediastinum, and Pneumopericardium” Cureus, vol 10, pp. 2861, 2018. doi: 10.7759/cureus.2861.


