Too Much Air in There
1 Division of Pulmonary Medicine, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH. 2Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH.
Case:
A former full-term 3-month-old with pectus excavatum presented to her primary pediatrician with worsening tachypnea and poor weight gain. She was referred to the emergency department after the chest radiograph shown below was obtained. On initial evaluation she had normal saturations on room air, but her respiratory rate was in the 70s and she had subcostal and suprasternal retractions on exam. Auscultation revealed diminished left sided aeration, but no wheezing, crackles, or other localized findings.

Figure 1: Supine Chest X-Ray
Question:
What is the diagnosis?
- Foreign body aspiration
- Congenital lobar emphysema
- Congenital pulmonary airway malformation
- Obstructive bronchogenic cyst
- Poland Syndrome
B. Congenital lobar emphysema
Discussion:
The answer is congenital lobar emphysema (CLE). The chest X-ray demonstrates classic findings of unilateral hyperlucency caused by overdistention of the affected lobe, mediastinal shift, and atelectasis of the contralateral lung (1).The findings seen here were also demonstrated on CT scan (below) which showed focal narrowing of the left upper lobe bronchus near its origin, with left lung overinflation resulting in rightward shift of the mediastinum. The infant in this case underwent flexible bronchoscopy to rule out a foreign body or another obstructive lesion prior to having a successful lobectomy. She recovered well and had resolution of tachypnea as well as improved weight gain.
CLE is a rare congenital lung malformation in which partial bronchial obstruction results in hyperinflation of one or more pulmonary lobes (1,2). CLE is also referred to as congenital lobar hyperinflation, infantile lobar emphysema, congenital large hyperlucent lobe, polyalveolar lobe, and congenital alveolar overdistention. Typical presentation is characterized by progressive tachypnea, respiratory distress, wheeze, recurrent respiratory infections, and failure to thrive (1,2). The diagnosis of CLE is difficult prenatally, but almost all cases are diagnosed prior to 6 months of age with 50% diagnosed in the immediate neonatal period (1-4). Though rare, presentation in adults has been described (5). Outside of the neonatal period insidious onset of symptoms is the norm and some patients may even remain asymptomatic (3). The left upper lobe is most commonly affected followed by the right middle lobe and right upper lobe; involvement of lower lobes is uncommon (1-3). The etiology is variable, and cases can generally be classified as resulting from internal bronchial obstruction, external bronchial obstruction, or a deficiency of the bronchial cartilage (1-3). About 50% of cases have no identifiable cause (2). CT or MRI with or without bronchoscopy is often used to confirm the diagnosis after CLE is suspected based upon chest X-ray. Treatment is based upon severity of clinical symptoms and consists of either surgical lobectomy or expectant management for asymptomatic and minimally symptomatic patients (1-4). Except in the rare and unique case of polyalveolar lobe which has true alveolar hyperplasia, histological examination shows normal radial alveolar counts with prominent airspace enlargement and no tissue damage as might be seen in acquired emphysema (1,2).
References
-
Abel, Robin M, et al. “Congenital Lung Disease.” Kendig and Chernick's Disorders of the Respiratory Tract in Children, 8th ed., Elsevier, 2012, pp. 317–357.
-
Demir, Omer Faruk et al. “Congenital lobar emphysema: diagnosis and treatment options.” International journal of chronic obstructive pulmonary diseasevol. 14 921-928. 1 May. 2019, doi:10.2147/COPD.S170581
-
Kunisaki, Shaun M et al. “Current operative management of congenital lobar emphysema in children: A report from the Midwest Pediatric Surgery Consortium.” Journal of pediatric surgeryvol. 54,6 (2019): 1138-1142. doi:10.1016/j.jpedsurg.2019.02.043
-
Abdel-Bary, Mohamed et al. “Clinical and surgical aspects of congenital lobar over-inflation: a single center retrospective study.” Journal of cardiothoracic surgeryvol. 15,1 102. 19 May. 2020, doi:10.1186/s13019-020-01145-8
-
Shen, Cheng, and Guowei Che. “Congenital Lobar Emphysema in an Elderly Patient.” American journal of respiratory and critical care medicine, 10.1164/rccm.202004-1337IM. 8 Sep. 2020, doi:10.1164/rccm.202004-1337IM
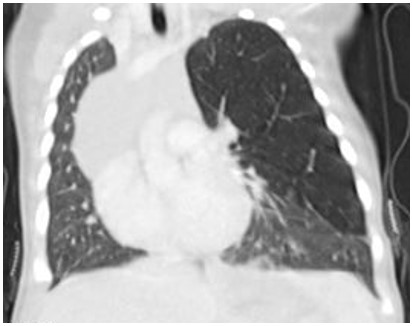
Figure 2: Coronal CT scan

Figure 3: Axial CT Scan


