Contributed by Dagmar Lin, MD, Shirin Shafazand, MD, MS, Department of Medicine, Division of Pulmonary Critical Care & Sleep Medicine University of Miami, Miller School of Medicine, Douglas M. Wallace, MD, Department of Neurology, Sleep Medicine Division University of Miami, Miller School of Medicine
A 42 year old man reported fever up to 104°F (40°C) and altered mental status 2 days after returning from a Caribbean cruise. He had been bitten by mosquitoes on the last day of the trip. Upon returning home, he developed headaches, lethargy, hypersomnia (sleeping 14-18 hours a day), episodes of confusion, and occasional word finding difficulty.
After 3 days of symptoms, he was hospitalized. On exam, he was febrile with meningeal signs, somnolent, oriented to self, expressive aphasia, but otherwise non-focal. Cerebrospinal fluid revealed lymphocytes (88/ml), protein (72 mg/dl), and normal glucose. He received empiric treatment with acyclovir and IV antibiotics. CSF cultures showed no growth. Past medical history was non-contributory.
Enhanced brain MRI was unremarkable and 24-hour EEG showed intrusion of bi-frontal theta waves without epileptiform activity. Tests for other infectious or metabolic etiologies were unremarkable. He continued to have persistent fatigue and hypersomnia 3 months after discharge. He also developed binge-eating episodes, gained 20 lbs and had loss of libido.
The patient was referred to our sleep clinic for evaluation. He denied sleep paralysis or cataplexy symptoms. Mild sleep apnea was diagnosed by attended in lab polysomnography (PSG). No periodic limb movements (PLMs) were detected. Table 1 shows baseline sleep architecture. The Apnea-Hypopnea Index (AHI) was 8 events/h (Figure 1). He underwent positive airway titration study and continuous positive airway pressure (CPAP) was prescribed at 10 cm H20. After 5 months of CPAP therapy with excellent objective adherence (9 hours per night), he continued to complain of hypersomnia. Actigraphy was performed using a Respironics Spectrum actigraph. Mean sleep duration in a 24 hour period, over 15 days of monitoring was 11.2 ± 3.1 hours. Repeat PSG confirmed adequate treatment of sleep disordered breathing and was followed by a MSLT (Table 2).
Figure 1: Summary of Baseline PSG
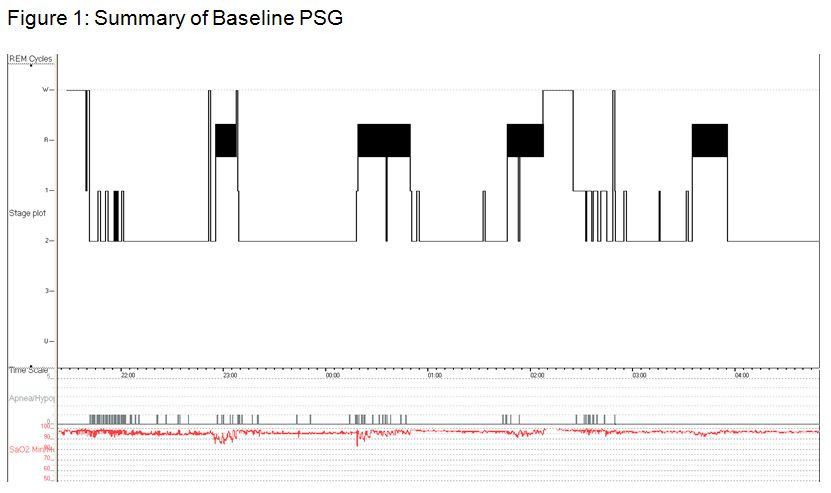
Table 1: Baseline Sleep Architecture
Metric |
|
|
Total Sleep Time (TST), min |
426 |
|
Sleep Efficiency |
87% |
|
Wake After Sleep Onset (WASO), min |
32.5 |
|
Sleep Onset Latency (SOL), min |
23.0 |
|
Latency to Stage REM, min |
81.0 |
|
N1, %TST |
7.2 |
|
N2, %TST |
76.1 |
|
N3, %TST |
0 |
|
R, %TST |
16.7 |
Table 2: Multiple Sleep Latency Test (MSLT)
MSLT |
Sleep Latency (min) |
REM Latency (min) |
|
Nap 1 |
11.0 |
N/A |
|
Nap 2 |
2.5 |
N/A |
|
Nap 3 |
7.0 |
10.5 |
|
Nap 4 |
6.5 |
9.5 |
|
Mean |
6.75 |
NA |
Question
What is the most likely diagnosis?
A) Poorly Controlled Sleep Disordered Breathing
B) Idiopathic Hypersomnia
C) Narcolepsy without Cataplexy
D) Insufficient Sleep
Answer
The most likely diagnosis is C) Narcolepsy without Cataplexy1
Discussion
The headache, behavioral changes, fatigue, expressive aphasia, and meningeal signs beginning after mosquito bites together with an antibiotic-resistant illness, focal EEG changes suggests a diagnosis of viral meningoencephalitis. As with many cases of viral meningoencephalitis, the etiology could not be determined.
Persistent hypersomnia despite five months of excellent CPAP adherence raised the suspicion of another co-morbid sleep disorder. MSLT after repeat overnight PSG with CPAP revealed 2 sleep-onset rapid eye movement periods (SOREMPs) and shortened mean sleep latency < 8 minutes in duration. The patient had adequate sleep duration based on 15 days of actigraphy, no evidence of PLMs and no medication use that could account for MSLT results. This case presentation is most consistent with hypersomnia of central origin, and given the specific findings on MSLT is likely attributed to narcolepsy.
Although rare, narcolepsy or narcolepsy-like presentations can be seen in a wide range of medical and neurological disorders, collectively termed symptomatic or secondary narcolepsy. These include neurodegenerative disorders (Parkinson’s disease), inflammatory and infectious diseases (multiple sclerosis, paraneoplastic encephalitis, viral encephalitis), and vascular events (hypothalamic, median thalamic or pontine strokes). Neoplasms with hypothalamic and/or mesenphalic involvement and head trauma are the two of the most common etiologies of symptomatic narcolepsy.2,3
There have been case reports of narcolepsy in the context of meningoencephalitis.2 Von Economo was the first to describe the neuropathological findings of posterior hypothalamic lesions in the brain of patients with the hypersomnolent variant of encephalitis lethargica (following the Spanish flu pandemic).3 Narcolepsy can be observed immediately or up to 6 months after acute encephalitis. Neuro-invasive viral infections may produce narcolepsy by damaging the hypothalamus, thalamus or other wake-promoting regions. Streptococcal infections have been implicated as an important environmental trigger for narcolepsy.4 Additionally, recent reports of increased incidence of narcolepsy post Pandemrix HINI vaccination in children are intriguing.5,6 The loss of hypothalamic orexin producing neurons causes narcolepsy with cataplexy. An autoimmune basis for this destruction has long been suspected. Much is unknown about the underlying mechanisms of infection associated narcolepsy. HINI vaccination, streptococcal or viral infections may initiate a specific immune response and subsequently perpetuate the autoimmune destruction of hypothalamic neurons through molecular mimicry or alternatively, trigger a non-specific immune activation that precipitates the disease in predisposed individuals.
In our patient, lesions were not visualized on neuro-imaging studies but he displayed clinical signs of hypothalamic dysfunction (sleepiness, eating dysregulation, weight gain, and libido loss). This is suggestive of destruction of orexin producing neurons and may be the cause of narcolepsy in this patient.
References
- American Academy of Sleep Medicine: International Classification of Sleep Disorders, 2nd ed. Diagnostic and Coding Manual. Westchester, IL: American Academy of Sleep Medicine, 2005.
- Nishino S, Kanbayashi T. Symptomatic narcolepsy, cataplexy and hypersomnia, and their implications in the hypothalamic hypocretin/orexin system. Sleep Med Rev 2005; 9(4): 269-310.
- Kanbayashi T, Sagawa Y, Takemura F, Ito SU, et al. The pathophysiologic basis of secondary narcolepsy and hypersomnia. Curr Neurol Neurosci Rep 2011; 11(2): 235-241.
- Aran A, Lin L, Nevsimalova S, Plazzi G, et al. Elevated anti-streptococcal antibodies in patients with recent narcolepsy onset. Sleep 2009; 32(8): 979-983.
- Nohynek H, Jokinen J, Partinen M, Vaarala O, et al. AS03 adjuvanted AH1N1 vaccine associated with an abrupt Increase in the incidence of childhood narcolepsy in Finland. PLoS ONE 2012; 7(3): e33536 doi:10.1371/journal.pone.0033536
- Han F, Lin L, Warby SC, Faraco J, Li J, et al. Narcolepsy onset is seasonal and increased following the H1N1 epidemic in China. Annals of Neurology 2011; 70: 410-417.
- Kornum B, Faraco J, Mignot E. Narcolepsy with hypocretin/orexin deficiency, infections and autoimmunity of the brain Current Opinion in Neurobiology 2011; 21:897-903.


