Contributed by Indra Narang, MD. The Hospital For Sick Children, Toronto, ON, Canada.
Background:
A 6 year old boy presented with an abdominal mass. His past medical history was non-significant. During routine observations during the night, he was noticed to have intermittent oxygen desaturations.
On examination, he was afebrile. He was thriving. His weight and height were both on the 50th percentile. His oxygen saturations while awake were 97% in room air. Other than a left sided abdominal mass, his cardiovascular, respiratory, neurological and developmental examinations were normal.
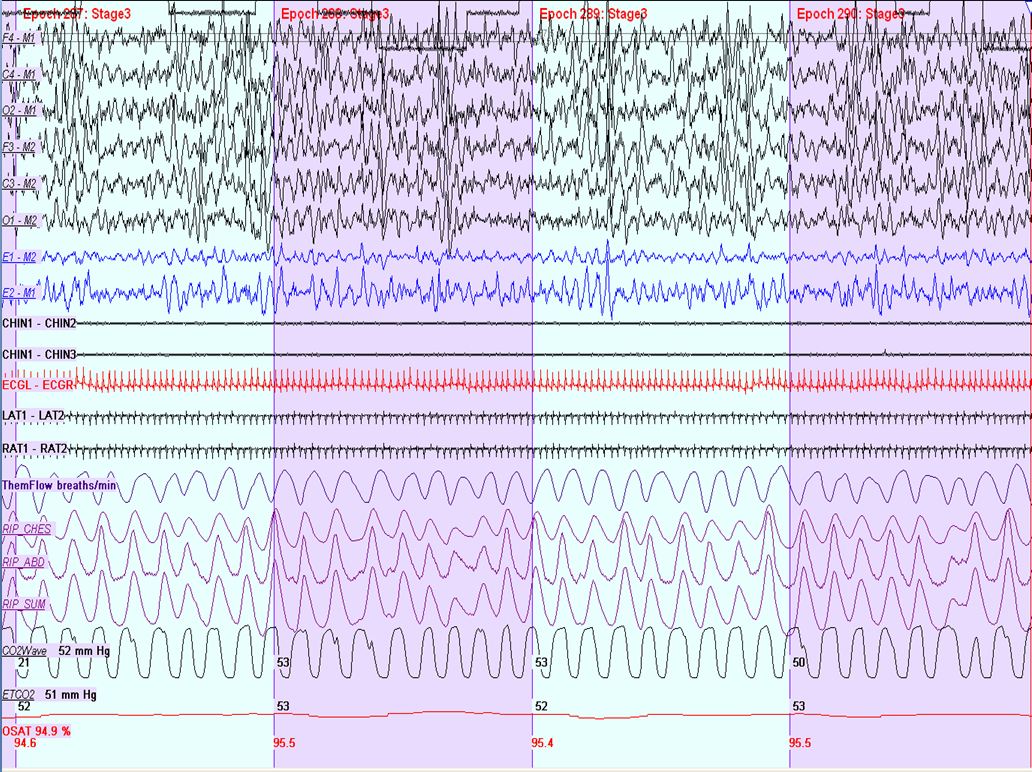
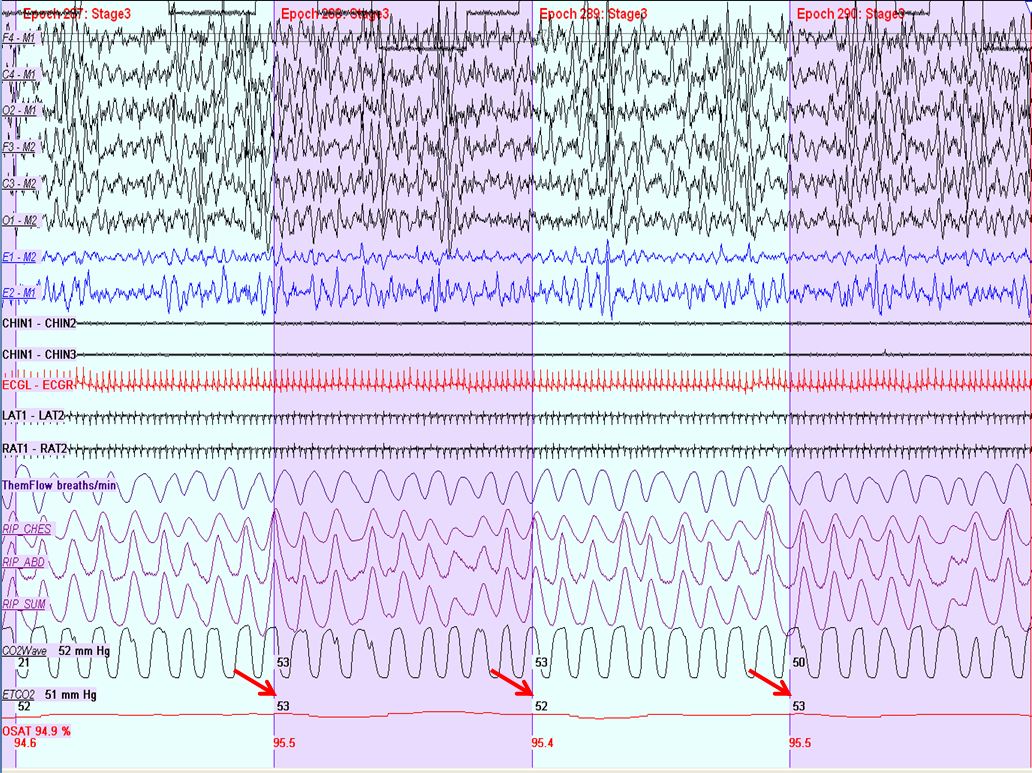
An overnight polysomnography (PSG) was performed to evaluate his intermittent nocturnal desaturations. A representative 2 minute tracing of his PSG is shown here.
Questions:
- What is the abnormal finding on this PSG?
- What diagnosis would you consider in this boy?
Answer:
- End-tidal CO2 > 50mmHg in the absence of any respiratory events during slow wave sleep.
- Late onset congenital central hypoventilation syndrome (LO-CCHS)
Discussion:
- The full PSG of this subject revealed an end-tidal CO2 of > 50mmHg for 80% of the night (highest recorded CO2 was 58 mmHg), with intermittent oxygen desaturations to 83% in the absence of respiratory events. The average respiratory rate of this subject was 12 per minute. The central apnea index was < 1.0/hour. These CO2 findings are consistent with a diagnosis of nocturnal hypoventilation, defined as an end-tidal or transcutaneous CO2 of > 50mmHg for 25% of the night (1). Further investigations in this child revealed he had a left sided adrenal gland neuroblastoma. Genetic analysis revealed he was heterozygous for a deletion of the single nucleotide at position 710 of the Phox2B gene resulting in a stop codon mutation, confirming CCHS. The child subsequently underwent successful treatment for his neuroblastoma and he was also commenced on nocturnal bilevel positive airway pressure therapy for treatment of nocturnal hypoventilation.
- CCHS subjects lack an adaptive ventilatory and appropriate arousal responses during sleep with a resultant decrease in minute ventilation. Specifically, these patients lack a ventilatory response to hypercapnia and consequently, these subjects will demonstrate nocturnal hypoventilation. PSG findings of CCHS patients typically demonstrate more severe alveolar hypoventilation and a higher frequency of central apneas during non-REM sleep (2). While awake, CCHS subjects lack a perception of dyspnea but maintain conscious control of breathing. Furthermore, CCHS is associated with autonomic nervous system dysfunction, Hirschprungs disease and neural crest tumours (3).
- CCHS was originally believed to present solely in the newborn with unexplained respiratory failure, cyanosis and acute life threatening episodes. However, LO-CCHS is now frequently described in childhood and adulthood with subjects presenting with unexplained oxygen desaturations, hypoventilation and/or respiratory failure following sedation, anaesthesia or a pneumonic episode. The diagnosis may be suspected with history and an abnormal PSG.
- CCHS is defined by clinical testing and confirmed with genetic testing for Phox2B mutations. Phox2B promotes neuronal differentiation and development of the autonomic nervous system. Phox2B is located at 4p12 and normally contains a 20-alanine repeat sequence (genotype 20/20). Individuals with CCHS are heterozygous for a Phox2B mutation, with the vast majority having a polyalanine repeat expansion mutation (PARM). The range for number of repeats in the Phox2B polyalanine expansion on the affected allele in patients with CCHS is 24–33 accounting for 90–92% of CCHS cases (3).
- The remainder of the CCHS Phox2B mutations results from misense, nonsense, frameshift or stop-codon mutations and are referred to as non-PARMS (NPARMS).
- Some phenotype/genotype correlations exist. Subjects carrying the shortest alanine repeats (20/24 and 20/25) typically display a less severe phenotype and it is these subjects who may present with LO-CCHS. The respiratory phenotype is generally more severe in patients with longer polyalanine expansions. Indeed, animal models expressing the Phox2B 20/27 allele disrupt the retrotrapezoid nucleus, located in the reticular formation which plays a key role in chemosensitivity. Such disruptions in the retrotrapezoid nucleus are linked with lack of respiratory response to hypercapnia in these animals (4).
Further Hirschsprungs disease does not typically occur with the shortest expansions while sympathetic-adrenal system tumours are more frequent with Phox2B frameshift or missense mutations.
References
- Iber C, Ancoli-Israel S, Chesson A, Quan SF. The AASM manual for the scoring of sleep and associated events: rules, terminology, and technical specifications, 1st ed. Westchester, IL: American Academy of Sleep Medicine; 2007.
- Huang J, Colrain IM, Panitch HB, Tapia IE, Schwartz MS, Samuel J, Pepe M, Bandla P, Bradford R, Mosse YP, Maris JM, Marcus CL. Effect of sleep stage on breathing in children with central hypoventilation. J Appl Physiol 2008;105:44-53.
- Weese-Mayer DE, Berry-Kravis EM, Ceccherini I, Keens TG, Loghmanee DA, Trang H. An official ATS clinical policy statement: Congenital central hypoventilation syndrome: Genetic basis, diagnosis, and management. Am J Respir Crit Care Med 2010;181:626-644.
- Ramanantsoa N, Hirsch MR, Thoby-Brisson M, Dubreuil V, Bouvier J, Ruffault PL, Matrot B, Fortin G, Brunet JF, Gallego J, Goridis C. Breathing without co(2) chemosensitivity in conditional phox2b mutants. J Neurosci 2011;31:12880-12888.


