Contributed by Katherine A. Dudley 1, Sanjay R. Patel 2; 1) Harvard Combined Pulmonary Fellowship Program, Harvard Medical School, Boston, MA, 02115, USA 2) Division of Sleep Medicine, Brigham and Women’s Hospital, Boston, MA, 02115, USA
A 77 year old man underwent overnight oximetry to assess severity of nocturnal desaturations after discontinuing CPAP therapy due to intolerance. His underlying medical conditions include ischemic cardiomyopathy, with left ventricular ejection fraction estimated at 35%, obesity, and hypertension. A sleep study greater than one year ago demonstrated severe sleep disordered breathing with AHI of 103 and oxygen saturation nadir of 67%. On examination in clinic, notable findings included presence of obesity, irregular heart beat, and trace peripheral edema.
Images:
Below is a portion of his home based overnight oximetry. Hash-marks denote 5 minute time increments.
Figure 1: Oximetry on supplemental oxygen alone
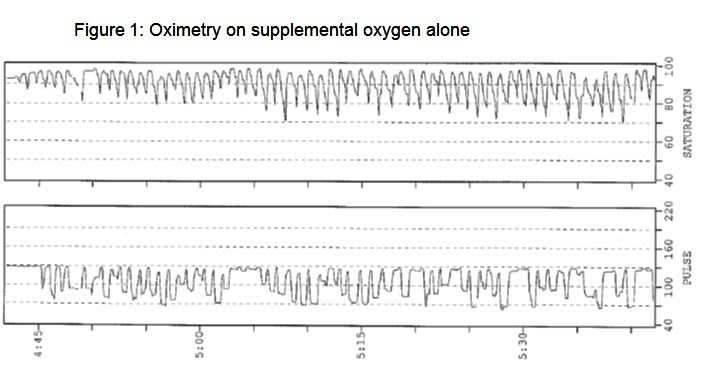
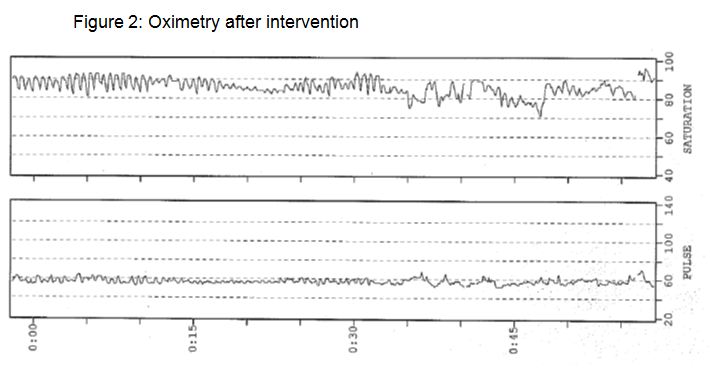
Figure 2: Oximetry after intervention
1. The above oximetry tracing is suggestive of what type of underlying sleep disordered breathing?
A. REM-related hypoventilation
B. Obstructive sleep apnea
C. Cheyne-Stokes respiration
D. Opiate-induced central sleep apnea
2. What intervention would account for changes seen on repeat oximetry?
A. Ablation of atrial flutter
B. Increase in supplemental oxygen
C. Initiation of furosemide
D. Lateral sleep
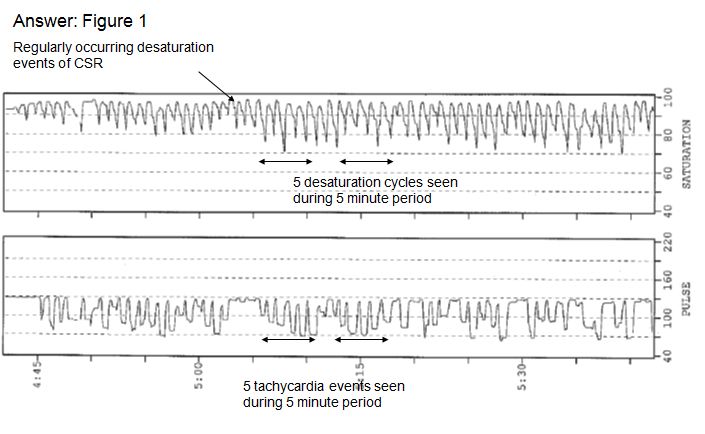
Question 1: C
The oximetry tracing is suggestive of underlying Cheyne-Stokes respirations with regular, repetitive desaturations of similar duration and severity. There is also marked heart rate variability.
Figure 1 with annotation
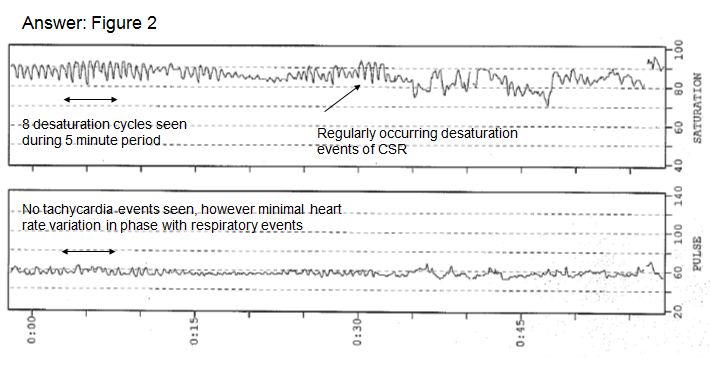
Question 2: A
Intervention was ablation of atrial flutter; patient did not have evidence of significant volume overload. Tracing shows fewer heart rate excursions and change in frequency of respiratory events.
Figure 2 with annotation
Discussion
Cheyne-Stokes respiration (CSR) is characterized by a repetitive, crescendo-decrescendo pattern of tidal volume changes and associated central apneas. CSR and central sleep apnea are commonly seen in patients with underlying left ventricular dysfunction, with prevalence estimated at 40% or greater (1). CSR may be present despite optimization of congestive heart failure regimen and absence of daytime sleepiness. Atrial fibrillation is an independent predictor of CSR in those with heart failure (2).
The breathing pattern of CSR may entrain the ventricular response to atrial fibrillation by influencing both the refractory period as well as concealed conduction at the level of the atrioventricular (AV) node resulting in a reduced ventricular response during apnea and increased response during hyperpnea (3). This effect appears to be mediated through autonomic changes and unlike the oscillations in heart rate commonly seen in obstructive sleep apnea, appears independent of baroreceptor reflexes (3).
In our case, the initial oximetry tracing demonstrates desaturation events at a frequency of approximately 5 cycles per 5 minutes, or 1 Hertz (Hz). Duration of CSR events is directly proportional to circulation time and indirectly proportional to cardiac output, demonstrated by Ryan and Bradley, building on prior observations (4).
An additional observation in the initial tracing is the oscillation frequency of about 1 Hz in heart rate, which is similar to the CSR frequency and suggests respiratory entrainment of the ventricular response to the atrial tachycardia.
Repeat oximetry after ablation of atrial flutter demonstrates desaturations at a frequency of about 8 cycles per 5 minutes (1.6 Hz), consistent with more rapid cycling. Heart rate variability is much less pronounced with a stable rate of about 60 beats per minute. Laboratory polysomnography confirmed the patient continued to have CSR despite remaining in normal sinus rhythm. The increased desaturation frequency on overnight oximetry reflects an improvement in cardiac output and thus a shorter lung-to-chemoreceptor circulatory delay. With more rapid sensing of changes in pCO2, the cycle length of CSR shortens and the frequency increases. The patient was successfully treated using adaptive-servo-ventilation after the ablation procedure.
This case highlights the wealth of information potentially available through overnight oximetry.
References
(1) Javaheri S, Parker TJ, Liming JD, Corbett WS, Nishiyama H, Wexler L, Roselle GA. Sleep apnea in 81 ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations. Circulation 1998;97(21):2154-9
(2) Blackshear JL, Kaplan J, Thompson RC, Safford RE, Atkinson EJ. Nocturnal dyspnea and atrial fibrillation predict Cheyne-Stokes respirations in patients with congestive heart failure. Arch Intern Med 1995: 1297-1302
(3) Leung RS, Bowman ME, Diep TM, Lorenzi-Filho G, Floras JS, Bradley TD. Influence of Cheyne-Stokes respiration on ventricular response to atrial fibrillation in heart failure. J Appl Physiol 2005;99(5):1689-96
(4) Ryan CM, Bradley TD. Periodicity of obstructive sleep apnea in patients with and without heart failure. CHEST 2005;127:536-542


