Contributed by S. H. Launois, MD PhD1-2, J.P. Fresco, MD2, 1 Grenoble University Hospital, Sleep Disorders Centre and INSERM U1040 HP2 Laboratory, Joseph Fourier University, Grenoble, France 2 Sleep Health Centre, Grenoble, France
A 46 year old woman presented to the Sleep Clinic with a complaint of severe insomnia dating back at least ten years. She stated that she hardly ever slept, at least never more than 3 hours a night. She reported constant mental activity during the night. The patient’s thoughts revolved around the past and upcoming work day, her family life as well as current events in the news. She had taken various hypnotic drugs over the last two years and eventually stopped because of lack of efficacy. In spite of this profound insomnia, the patient reported mild fatigue but no significant daytime sleepiness (Epworth sleepiness score = 9/24) and no cognitive dysfunction. She was not on any medication. Caffeine intake was limited to one cup of coffee in the morning.
Significant medical history included severe depression two years prior to the initial sleep assessment, with successful treatment with antidepressant medication and psychotherapy, which had been discontinued after a year.
The patient was reluctant to keep a sleep log, stating that "she never slept at all anyway". Thus, only home polysomnography (PSG) and actimetry were obtained. This testing was obtained during a week of scheduled vacation when she stated that she had tried to sleep longer at night, by later rising and by napping during the afternoon, with no success. The PSG was recorded on the first night of the week, when the patient reported that she had slept less than one hour during the night.
The PSG hypnogram is shown in Image 1 and sleep parameters are presented in the table. The actimetry results are shown in Image 2.
What is the diagnosis?
- Inadequate sleep hygiene
- Psychophysiological Insomnia
- Paradoxical Insomnia
- Circadian rhythm sleep disorder
Images
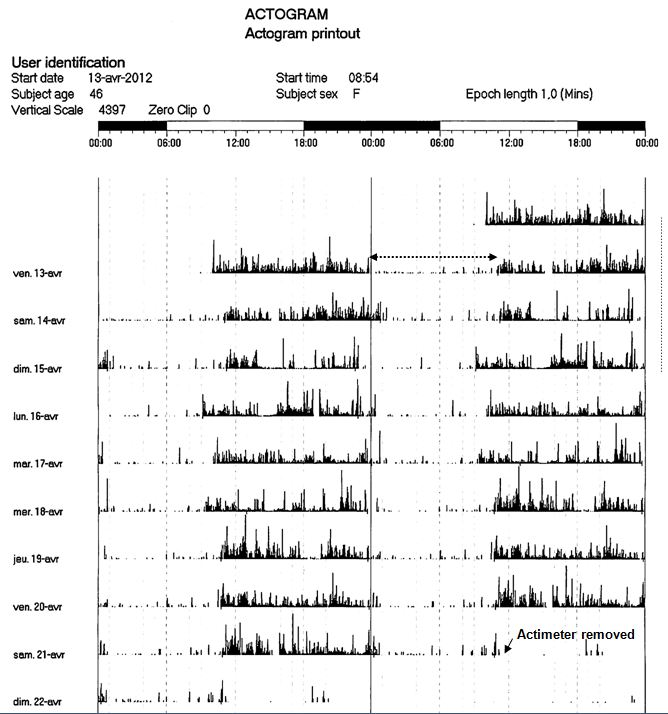
Image 1: Patient’s PSG hypnogram for the night of April 13 (dotted line on Image 2). EVEIL = wakefulness; SP = Rapid Eye Movement sleep, 1 = stage N1; 2 = stage N2; 3 = stage N3.
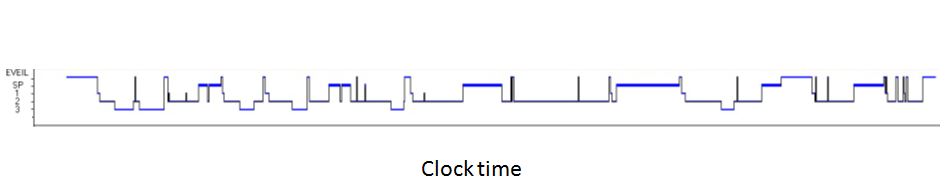
Image 2: Patient’s double plot actigram recorded during a one-week vacation. Recordings were made at one minute periods. The second cycle on a line is the same as the first cycle on the following line. Home polysomnography was performed on the night of April 13 (dotted arrow).
Table:
|
PSG sleep parameters
|
|
|
TST |
485 min |
|
Sleep efficiency |
92% |
|
Sleep latency |
19 min |
|
REM sleep latency |
64 min |
|
Arousals |
29/hr |
|
WASO |
40 min |
|
N1 |
14 min (2.9% TST) |
|
N2 |
285 min (58.8% TST) |
|
N3 |
63 min (13% TST) |
|
REM |
123 min (25.4% TST) |
|
PLM index |
5/hr |
|
AHI |
1/hr |
TST = total sleep time; WASO = wake after sleep onset. PLM = periodic leg movement; AHI = apnea hypopnea index
The patient suffers from paradoxical insomnia: the discrepancy between estimated sleep time and objective sleep time calculated on PSG (supported, in this case, by the results of actimetry) and the lack of daytime consequences of the drastic sleep loss reported by the patient are the essential features of this insomnia subtype.
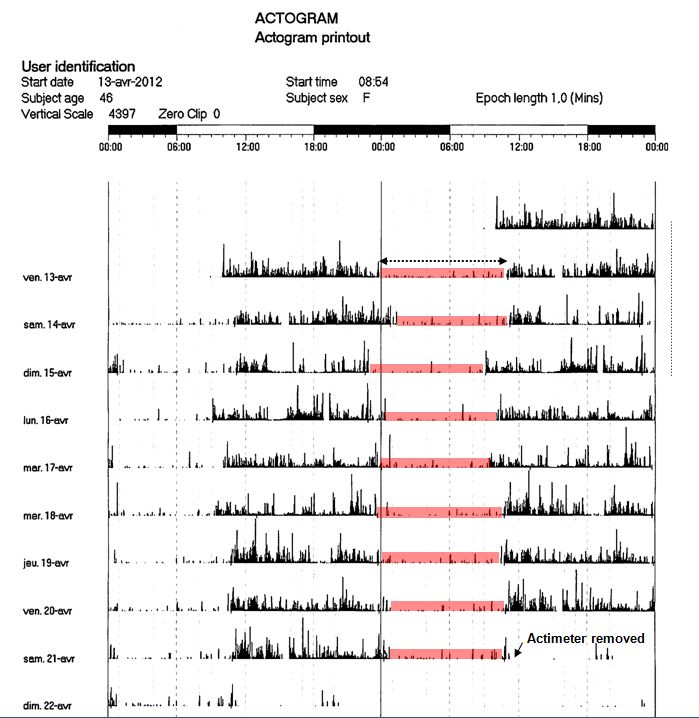
PSG analysis shows an objective total sleep time of 8 hours, while the patient reported an estimated sleep time that night of less than one hour. Additionally, actigram consistently shows nocturnal sleep periods of 8 hours or longer (highlighted in red).
Discussion
"Paradoxical insomnia" is a primary insomnia subtype introduced in the revised International Classification of Sleep Disorders in 2005 to replace the former "Sleep State Misperception" category.1 Paradoxical insomnia is characterized by a discrepancy between subjective sleep time and objective sleep evaluated by polysomnography (PSG) or actimetry, constant rumination and/or awareness of external stimuli during the night and a level of daytime impairment inconsistent with the reported sleep deprivation. Overestimation of sleep latency and wake after sleep onset and underestimation of total sleep time are common in most insomniacs, but in patients with paradoxical insomnia, the discrepancy between subjective and objective sleep is far greater.2 In the absence of adequate general population studies and given the variability in clinic-based study results, the prevalence is difficult to ascertain2 but it is probably low, paradoxical insomnia affecting less than 5% of insomniacs.1
In our patient, all ICSD-2 diagnostic criteria were present, although we were not able to convince the patient to keep a sleep diary. Because of the extreme sleep loss reported by the patient, the absence of daytime impairment and of symptoms suggestive of another type of insomnia, polysomnography and actimetry were recommended. Their results supported the initial clinical impression of sleep state misperception. Differential diagnoses include malingering and, particularly when the mismatch between subjective and objective measurements of sleep is less marked than in our patient, other types of primary insomnia such as psychophysiological or idiopathic insomnia.
Little is known about the mechanisms underlying sleep misperception. Although conventional sleep staging is not significantly different in normal sleepers and paradoxical insomniacs, more subtle abnormalities (stage 2 and 3 spectral measures, cyclic alternating patterns and arousals) have been reported and may contribute to the patient’s sensation of unrefreshing sleep, delayed sleep onset and increased WASO.2-5 Our patient indeed had several brief awakenings and the arousal index was relatively high (Image 1, Table). No clear cause for this sleep fragmentation could be established. There was no significant respiratory abnormality or periodic limb movements.
The patient was seen again in clinic to discuss the results of the PSG and the actimetry. She was relieved by our explanations and a follow-up visit was scheduled 6 months later. However, in our experience as well as others,2 some patients tend to be exceedingly dissatisfied with the diagnosis and blame PSG results on faulty sensors or incompetent sleep technologists. In such patients, relief of paradoxical insomnia is often difficult to achieve.
There are currently no guidelines regarding treatment options. Rather than improving sleep habits or prescribing a course of sedative medication, improving sleep perception through cognitive behavioral therapy may be more effective in these patients2, 6-7. Current published data on comparing various interventions are scant. The management error in these patients is prescribing a sedative hypnotic at bedtime with increasing dosage as was the case in this patient with no improvement on follow-up evaluation, and increasing risk of daytime side effects. Fortunately, our patient had spontaneously discontinued her treatment because of the lack of efficacy. Objective evaluation of sleep, with actimetry and/or polysomnography should be considered when there is a lack of treatment efficacy in insomnia.
References
-
American Academy of Sleep Medicine. International classification of sleep disorders, ed 2. Westchester, IL: American Academy of Sleep Medicine; 2005.
-
Edinger JD, Krystal AD. Subtyping primary insomnia: Is sleep state misperception a distinct clinical entity? Sleep Med Rev 2003;7:203-214.
-
Smith S, Trinder J. The effect of arousals during sleep onset on estimates of sleep onset latency. J Sleep Res 2000;9:129-135.
-
Parrino L, Milioli G, De Paolis F, Grassi A, Terzano MG. Paradoxical insomnia: The role of cap and arousals in sleep misperception. Sleep Med 2009;10:1139-1145.
-
Turcotte I, St-Jean G, Bastien CH. Are individuals with paradoxical insomnia more hyperaroused than individuals with psychophysiological insomnia? Event-related potentials measures at the peri-onset of sleep. Int J Psychophysiol 2011;81:177-190.
-
Geyer JD, Lichstein KL, Ruiter ME, Ward LC, Carney PR, Dillard SC. Sleep education for paradoxical insomnia. Behav Sleep Med 2011;9:266-272.
-
Tang NK, Harvey AG. Correcting distorted perception of sleep in insomnia: A novel behavioural experiment? Behav Res Ther 2004;42:27-39.
Citation: Launois SH, Fresco JP. Ten years of sleepless nights. Ann Am Thorac Soc 2013;10:67-70.


