Contributed by Vinod Aiyappan1, Prashanthan Sanders2, Doug McEvoy1 Nick A Antic1, 1. Adelaide Institute for Sleep Health (AISH), Repatriation General Hospital, Daw Park, Adelaide, South Australia, Australia. 2. Centre for Heart Rhythm Disorder, University of Adelaide and Royal Adelaide Hospital, Adelaide, Australia.
A 76-year-old woman was referred for evaluation of snoring, witnessed apneic episodes and daytime tiredness. She was otherwise well except for hypertension for which she took telmisartan 80 mg daily.
The patient underwent a split night laboratory sleep study (baseline sleep evaluation followed by continuous positive airway pressure (CPAP) titration during one night of study). She took no sedating drugs and consumed no caffeinated beverages on the day prior to the overnight study.
A representative sample of her polysomnography (PSG 30 second epoch for ECG and EEG and 5 minute epoch for saturation trace, nasal pressure trace, thoracic and abdominal band traces) recorded during the diagnostic phase of the sleep study (Figure 1) is shown below.
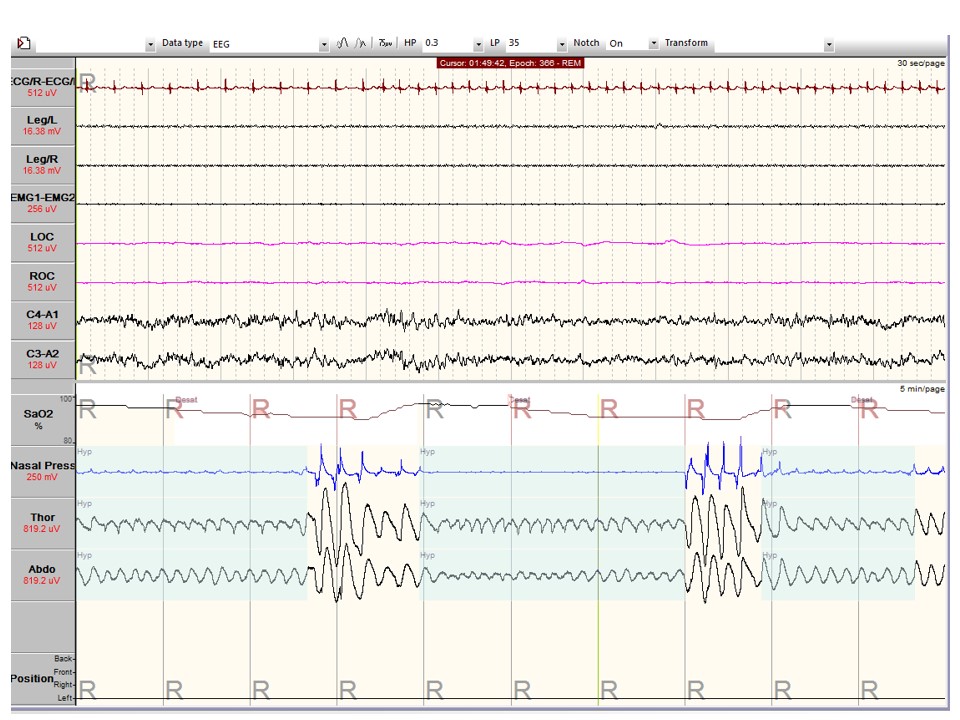
Figure 1: Representative recording from the diagnostic phase of the patient’s split night laboratory polysomnogram
Question
What abnormalities were recorded on the polysomnogram (Figure 1)?
Answer
The diagnostic PSG shows obstructive sleep apnea/hypopnea with associated oxygen desaturation. Figure 1 shows an additional abnormality that reinforces the importance of systematically reviewing all of the tracings included in a polysomnogram. The ECG recording shows abrupt onset of a narrow complex tachycardia associated with the respiratory event (Figure 2).
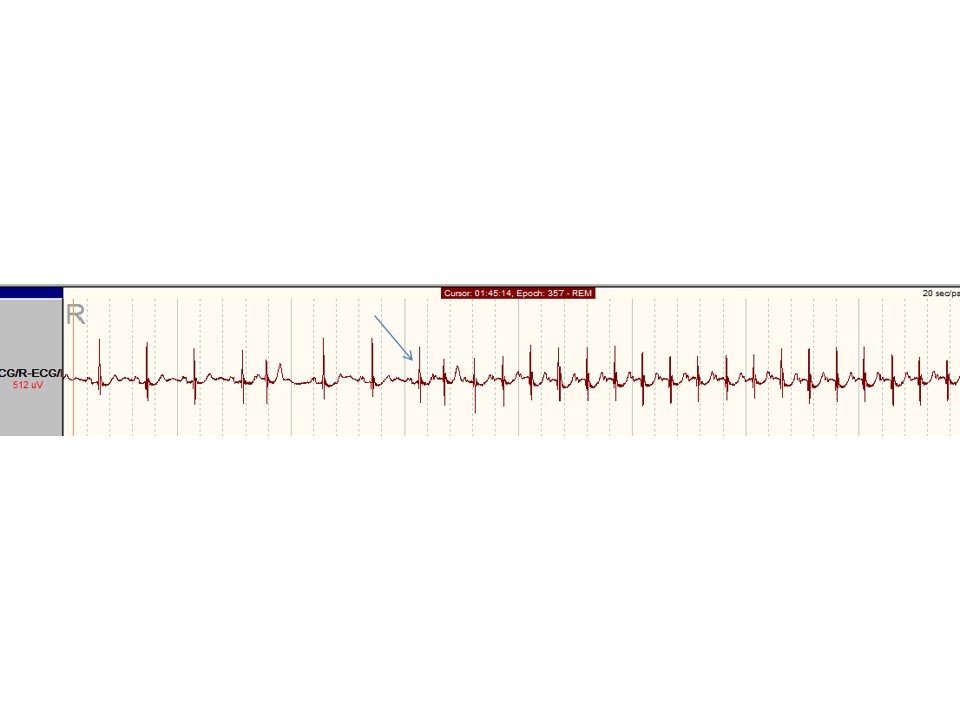
Figure 2: Expanded view of the ECG tracing from Figure 1 showing abrupt onset of a focal atrial tachycardia. Note the long RP interval.
Discussion
The diagnostic phase of the sleep study showed evidence of severe obstructive sleep apnea with an AHI of 33.7 and mild oxygen desaturation with a nadir of 87%. The respiratory flow disturbances, oxygen desaturations and runs of supraventricular tachycardia were largely abolished during the CPAP phase of the split night study.
The supraventricular tachycardia (SVT) noted during the patient’s PSG is a long RP (interval between the R wave and the P wave of the next cycle) tachycardia. The arrhythmia, although asymptomatic, was paroxysmal and frequent during the diagnostic phase of the study, and occurred in association with respiratory events. The heart rate rose to 110/minute during the arrhythmia from a baseline heart rate of 60/minute. A total of 92 episodes of paroxysmal atrial tachycardia were recorded during the diagnostic phase of the study (159.5 minutes), each lasting from 15 seconds up to 2 minutes. The CPAP titration portion showed only 2 short episodes of tachycardia.
A long RP tachycardia of sudden onset and termination with recurrent short bursts is characteristic of a focal atrial tachycardia. Other possibilities that could result in a long RP tachycardia include sinus tachycardia (which would have a more gradual onset and termination), accessory pathway related atrio-ventricular re-entrant tachycardia or atrio-ventricular junctional re-entrant tachycardia (the latter two usually being more sustained). While the tachycardia features are discernible on a single rhythm strip, prediction of the origin of the tachycardia focus is not possible without more ECG vectors.
The prevalence of obstructive sleep apnea (OSA) is increasing in the community1. The Sleep Heart Health Study (SHHS) demonstrated a higher prevalence of cardiac arrhythmias in patients with sleep disordered breathing (SDB)2. The relative risk of an arrhythmia is markedly higher after a respiratory disturbance during sleep, although the absolute arrhythmia rate is low3. Cardiac arrhythmias associated with OSA include bradycardia, tachycardia, AV block, increased atrial and ventricular ectopy, and supraventricular/ventricular tachyarrhythmias.
There are several possible mechanisms by which OSA predisposes to cardiac arrhythmias. The acute obstructive respiratory event in OSA results in repeated inspiratory effort against a closed glottis and produces negative intra-thoracic pressures which increases LV afterload and results in both direct and indirect stretch of the myocardium. Myocardial stretch is a potent stimulant for automatic activity resulting in development of an increased ectopy burden, and sustained automatic tachycardias (such as atrial tachycardias). This effect may be amplified by the profound fluctuations in autonomic stimulation and blood pressure that have been observed with acute obstructive events. In patients with an established abnormal atrial or ventricular substrate, such an increase in trigger burden may potentially initiate atrial fibrillation (AF) or ventricular tachycardia, respectively.
Our recent work demonstrates that patients with chronic repetitive obstruction may progress to electrical and structural remodelling of the atria to create this substrate for atrial fibrillation 5. Thus, in the patient with OSA, the acute obstructive episode may provide the milieu to trigger AF, while persistent and untreated OSA may result in chronic substrate contributing to the maintenance of AF which over time may contribute to mechanical and electrical remodeling5.
In addition to acute and chronic remodelling of the atria, there is repetitive and chronic sympathetic activation which also contributes to the development of arrythmia4,5. Others have highlighted the relative contributions of the fluctuations in hypoxia and hypercabia to the development of the acute electrical milieu predisposing to arrhythmia due to obstruction10.
The bradyarrythmias associated with OSA are attributed to the vagotonic effect of hypoxia, on the carotid body11. In addition to these mechanisms, atrial remodelling and the desaturation-resaturation cycle may activate atrial catecholamine sensitive ion-channels causing focal abnormal electric discharges contributing to the development of atrial arrythmias4,5,11,12. There is high prevalence of sleep apnea ( up to 87%) in patients with cardiac arrythmias14.
An earlier study demonstrated resolution of cardiac arrhythmias (AV block, sinus arrest, ventricular tachycardia, atrial flutter& atrial fibrillation) associated with sleep disordered breathing (SDB), after treatment with tracheostomy 6.
CPAP is an effective therapy for OSA and withdrawal of CPAP is associated with prolongation of cardiac repolarization, which could predispose to cardiac arrythmias7. Although a prospective study demonstrated that CPAP treatment is effective in controlling cardiac arrhythmias associated with OSA8, and observational studies have suggested a reduced recurrence of atrial fibrillation after treating OSA with CPAP, yet a randomized controlled trial (RCT) did not find any reduction in arrhythmias among OSA patients using CPAP, when compared to placebo9.
In summary, OSA is associated with increased risk of cardiac arrhythmias. The ECG of patients undergoing PSG should therefore be scrutinized for cardiac arrhythmias. Patients with cardiac arrhythmias should be assessed for symptoms and clinical features of underlying sleep disordered breathing and referred for sleep studies, when appropriate.
Follow-up
The patient’s thyroid function test results were normal. An echocardiogram did not reveal any structural cardiac abnormalities. Her symptoms resolved following initiation of nocturnal CPAP therapy.
References:
-
Adams R, Appleton S, Vakulin A, Taylor A, Martin S, Catcheside P, Antic A, McEvoy D, Wittert G. High prevalence of undiagnosed OSA in a community sample of men aged 40 years and over. Sleep and Biological Rhythms 2012;10 (suppl. 1):42
-
Mehra R, Benjamin EJ, Shahar E, et al. Association of nocturnal arrhythmias with sleep-disordered breathing. Am J Respir Crit Care Med 2006;173:910–6.
-
Mohanan K, Storfer-Isser A, Mehra R, Shahar E, Mittleman M,Rottman J,Punjabi N, Sanders M, Quan SF, Resnick, H, Redline S. Triggering of Nocturnal Arrhythmias by Sleep-Disordered Breathing Events. J. Am. Coll. Cardiol. 2009;54;1797-1804.
-
Ludka O, Konecny T, Somers V. Sleep Apnea, Cardiac Arrhythmias, and Sudden Death. Tex Heart Inst J. 2011; 38(4): 340–343
-
Dimitri H, Ng M, Brooks AG, Kuklik P, Stiles MK, Lau DH, Antic N, Thornton A, Saint DA, McEvoy D, Antic R, Kalman JM, Sanders P. Atrial remodeling in obstructive sleep apnea: implications for atrial fibrillation. Heart Rhythm. 2012 Mar;9(3):321-7.
-
Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndrome. Am J Cardiol. 1983 Sep 1;52(5):490-4.
-
Rossi VA, Stoewhas AC, Camen G, Steffel J, Bloch KE, Stradling JR, Kohler M. The effects of continuous positive airway pressure therapy withdrawal on cardiac repolarization: data from a randomized controlled trial. Eur Heart J. 2012 ;33(17):2206-12.
-
Harbison J, O'Reilly P, McNicholas WT. Cardiac rhythm disturbances in the obstructive sleep apnea syndrome: effects of nasal continuous positive airway pressure therapy. Chest. 2000 Sep;118(3):591-5
-
Craig S, Pepperell JC, Kohler M, Crosthwaite N, Davies RJ, Stradling JR. Continuous positive airway pressure treatment for obstructive sleep apnoea reduces resting heart rate but does not affect dysrhythmias: a randomised controlled trial. J Sleep Res. 2009;18(3):329-36.
-
Stevenson IH, Roberts-Thomson KC, Kistler PM, Edwards GA, Spence S, Sanders P, Kalman JM. Atrial electrophysiology is altered by acute hypercapnia but not hypoxemia: implications for promotion of atrial fibrillation in pulmonary disease and sleep apnea. Heart Rhythm. 2010 Sep;7(9):1263-70
-
Chen PS. Douglas P. Zipes Lecture. Neural mechanisms of atrial fibrillation. Heart Rhythm Nov;2006 3(11):1373–1377
-
Leung RS. Sleep-disordered breathing: autonomic mechanisms and arrhythmias. Prog Cardiovasc Dis. 2009 Jan-Feb;51(4):324-38.
-
Pinto JM, Garpestad E, Weiss JW, Bergau DM, Kirby DA. Hemodynamic changes associated with obstructive sleep apnea followed by arousal in a porcine model. J Appl Physiol. 1993 Oct;75(4):1439–1443
-
Hoyer FF, Lickfett LM, Mittmann-Braun E, Ruland C, Kreuz J, Pabst S, Schrickel J, Juergens U, Tasci S, Nickenig G, Skowasch D. High prevalence of obstructive sleep apnea in patients with resistant paroxysmal atrial fibrillation after pulmonary vein isolation. J Interv Card Electrophysiol. 2010 Oct;29(1):37-41.


