Contributed by Leila Kheirandish Gozal, MD, Associate Professor of Pediatrics, Director of Clinical Sleep Research, Section of Pediatric Sleep Medicine, Department of Pediatrics, The University of Chicago
A 4-year-old obese Caucasian boy is rushed to the emergency room by his mother after a long episode of seizure. He is found to be febrile to 103.8 F and his pulse oximetry values are 87%. His vitals signs reveal a blood pressure of 100/50 mmHg, heart rate of 112 beats/minute, a respiratory rate of 10 breaths/minute. His height and weight are 89 cm and 27.3 kg, respectively. While waiting for admission, the patient was given supplemental oxygen but stopped breathing and was intubated in the emergency room. He had cold extremities and was sweating profusely.
His past medical history indicates that his mother had a normal pregnancy. He weighed 3200 grams at birth with an Apgar score of 9. He was able to sit at 4 months of age and started walking by 11 months. At 38 months child had a sudden weight gain of 5 kg over a period of 3 months. He was put on a restricted calorie diet however in the following 4 months another 6 kg weight gain occurred.
The patient also had been complaining of diffuse abdominal pain for the past few weeks. In the last 2 months, he was very sleepy during the day even though he went to bed early every night. He snored loudly according to his mother and had been noticed to stop breathing at times during his sleep in the past year. The patient was also noticed to have mood changes and was seen by a child behavioral psychologist for the past 6 months. His mother believes that the seizure was due to severe dehydration since “he never remembers to drink enough water”.
In the hospital, a lumbar puncture test was performed and appeared normal yielding negative results for bacterial and viral culture; a chest radiograph was normal and sputum gram stain was also negative; a complete blood count revealed: a normal hemoglobin and hematocrit, and white blood cell count of 11,700, with 55% neutrophils and 22% lymphocytes. Electrolytes showed mild hyponatremia (Na: 132 mEq/L).
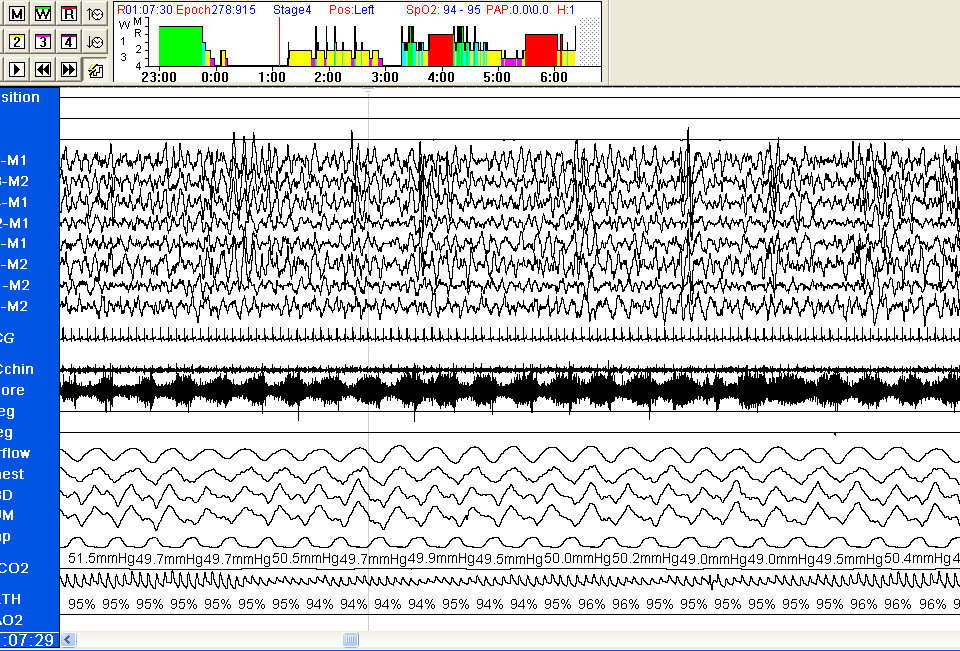
The morning after admission he was on minimal ventilator settings and was successfully extubated. However, he was noted to desaturate to the mid 80’s when he was asleep. A sleep study was, therefore, performed and revealed hypoventilation and an abnormal EEG with paroxysmal EEG activity in the absence of tonic-clonic seizures. His mean PETCO2 was 47 mmHg, with peak PETCO2 of 62 mmHg are noted along with recurrent desaturations to the mid 80s and nadir saturation of 67%. However, no evidence of obstructive respiratory events was apparent.
Question 1: What test would be most likely positive?
a-PHOX2B gene mutation
b-PHOX2B gene polyalanine expansion
c-RET proto-oncogene mutation
d-Methylation patterns within 15q11-q13 chromosome
e-None of the above
Question 2-What is the most likely diagnosis?
a-Congenital central hypoventilation syndrome
b-Prader–Willi syndrome
c-Angelman syndrome
d-Late Onset Central Hypoventilation Syndrome associated with Hypothalamic Dysfunction
ANSWER:
1) e - None of the above
2) d - Late Onset Central Hypoventilation Syndrome associated with Hypothalamic Dysfunction
DISCUSSION:
Rapid-onset Obesity with Hypothalamic dysfunction, Hypoventilation and Autonomic Dysregulation (ROHHAD syndrome) is a rare, complex disease with approximately 40 known cases worldwide, and was first described in 1965 as late-onset central hypoventilation with hypothalamic dysfunction by Fishman et al (1). A later paper on a case-series and review of the literature by Katz et al. (2) allowed for improved separation of this disorder from CCHS.
Symptoms are particularly related to autonomic and endocrine dysfunction, and may include hyperphagia and obesity, alveolar hypoventilation, altered respiratory control, cardiorespiratory arrest, reduced carbon dioxide ventilatory responses, obstructive sleep apnea, failed growth hormone stimulation, adipsic hypernatremia, hypernatremia, hyperprolactinemia, diabetes insipidus, gastrointestinal dysmotility, altered sweating, thermal dysregulation, water imbalance, pain hyposensitivity, behavioral disorders, strabismus, papillary anomalies, hyperprolactinemia, altered onset of puberty and tumors of neural crest origin, which can occur in 50% of cases (e.g. ganglioneuromas).
Unlike CCHS, which manifests in the newborn period with alveolar hypoventilation in the absence of primary lung, heart or neuromuscular abnormalities; ROHHAD presents exclusively after infancy (usually 1.5-7 years of age) and typically manifests as a sudden onset of hypothalamic dysfunction (rapid weight gain and obesity) followed by autonomic dysregulation and alveolar hypoventilation, usually preceded by what appears to be an acute intercurrent viral illness.
Diagnostic criteria:
Alveolar hypoventilation developing after the age of 2 years and evidence of hypothalamic dysfunction as defined by 1 or more of the following findings: rapid onset obesity, hyperprolactinemia, central hypothyroidism, disordered water balance, failed growth hormone stimulation test, corticotropin deficiency and delayed or precocious puberty (3).
Since the cause of this condition is unknown, there is no specific genetic test available for this disorder, and the diagnosis is based on the clinical presentation, the association of above mentioned clinical features, and exclusion of other potentially confounding diagnoses, particularly CCHS. To this effect, it is worthwhile noting that PHOX2B gene mutations are found in 91% and may approach 100% of the CCHS cases and that the symptoms in CCHS usually start very early in life.
Potential treatment options:
ROHHAD patients are complex and require a multidisciplinary team of specialists in order to secure their safety and well being.The obesity and hypothalamic dysfunction need to be thoroughly evaluated and treated by a team of pediatric endocrinologists and nutritionists. Hormone replacement, a strict fluid intake regimen, attention to conditions that may disrupt the unstable temperature regulation are all very important. In addition, depending on the severity of the central hypoventilation and associated hypoxemia, positive airway pressure ventilation may be needed either only at night or less frequently throughout the 24 hour period. To this effect, either nasal mask approaches or mechanical ventilation via tracheostomy are individually tailored to the patient. The potential development of neural crest tumors necessitates periodic monitoring as well.
References:
- Fishman LS, Samson JH, Sperling DR. Primary alveolar hypoventilation syndrome (Ondine’s curse). Am J Dis Child. 1965; 110:155–161.
- Katz ES, McGrath S, Marcus CL. Late-onset central hypoventilation with hypothalamic dysfunction: a distinct clinical syndrome. Pediatr Pulmonol. 2000;29:62–68.
- Ize-Ludlow D, Gray JA, Sperling MA, Berry-Kravis EM, Milunsky JM, Farooqi IS, Rand CM, Weese-Mayer DE. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation presenting in childhood. Pediatrics. 2007;120:e179-e188.


