Contributed by D. Testelmans, Leuven University Centre for Wake and Sleep disorders, University of Leuven, Leuven, Belgium, Grenoble University Hospital, Sleep Disorders Centre, Rehabilitation and Physiology Grenoble, France. J.L. Pépin, R. Tamisier, P. Lévy, Grenoble University Hospital, Sleep Disorders Centre, Rehabilitation and Physiology Grenoble, France
A polysomnography was performed.
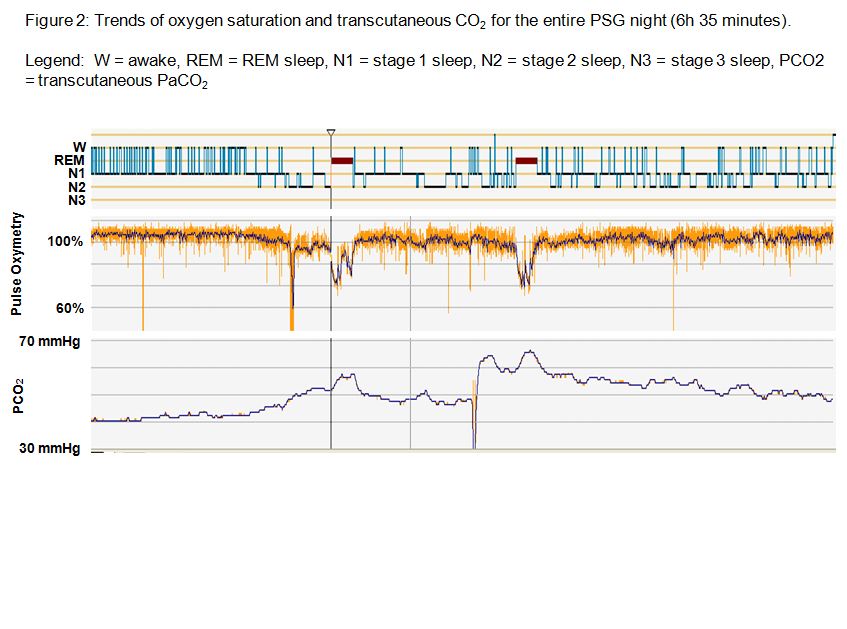
2. What does the overview of the full PSG show (Figure 2)?
3. Is the cardiovascular risk in the overlap syndrome (COPD and OSA) different from the risk in COPD?
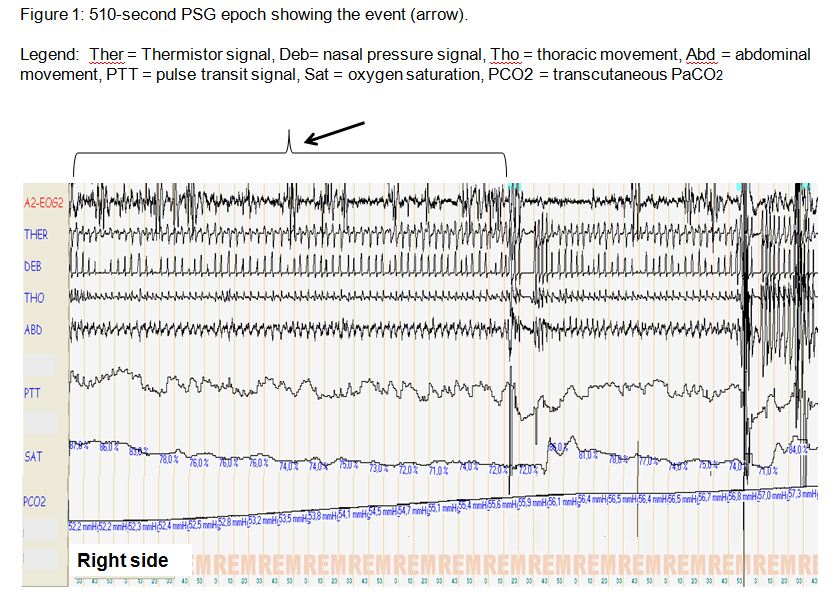
1) The arrow indicates an episode of alveolar hypoventilation during REM sleep.
2) The PSG shows some typical characteristics of sleep in patients with COPD: fragmented sleep with frequent awakenings or arousals, oxygen desaturation and hypercapnia which are more pronounced during REM sleep.
3) The cardiovascular risk in patients with overlap syndrome is increased in comparison with COPD patients without OSA.
Discussion:
The AASM manual for scoring of sleep and associated events (2007) defines hypoventilation as an event which is characterized by a > 10 mmHg increase in PaCO2 during sleep in comparison to an awake supine value [1]. The transcutaneous CO2 in our patient is clearly increased > 10 mmHg in comparison with the awake state.
During sleep, the drop in minute ventilation in COPD patients has been shown to be higher in comparison with healthy controls. This is largely due to a decrease in tidal volume. One possible explanation is an alteration of the respiratory drive to maintain preset minute ventilation during sleep [2]. Another possible explanation may be the increased dependence on accessory muscles which become hypotonic during sleep, particularly during REM sleep. Poor sleep quality in COPD patients has been documented by studies utilizing PSG, showing decreased total sleep time and decreased sleep efficiency, with the presence of many arousals [3].
In the present case, despite lack of daytime hypercapnia or significant hypoxemia, the patient exhibits demonstrative severe sleep-related hypoventilation episodes which are not unusual during REM sleep in patients with COPD. Moreover, these events are likely to be aggravated by obesity. However, daytime SaO2 is able to predict nocturnal oxygen desaturations in normoxic or mildly hypoxic patients with COPD, with nocturnal desaturations likely when daytime SaO2 is less or equal than 93% and unlikely when daytime SaO2 is more or equal than 95% [4].
This patient also had moderate OSA with an AHI of 22/h. Recognition of OSA in COPD is important, as recently, Marin et al. showed that as compared to patients with COPD alone, the overlap of OSA with COPD was associated with increased risk of cardiovascular deaths and of hospitalizations caused by COPD exacerbations. Furthermore, CPAP treatment could decrease these risks [5]. Hence, diagnosis and treatment of OSA in patients with COPD is warranted.
References:
1) Iber C et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. 2007, American Academy of Sleep Medicine: Westchester, Illinois
2) O’Donoghue FJ et al. Changes in respiration in NREM sleep in hypercapnic chronic obstructive pulmonary disease. J. Physiol 2004; 559: 663-673
3) Krachman SL et al. Effects of lung volume reduction surgery on sleep quality and nocturnal gas exchange in patients with severe emphysema. Chest 2005; 128: 3221-3228
4) Little SA, Elkholy MM, Chalmers GW, Farouk A, Patel KR, Thomson NC: Predictors of nocturnal oxygen desaturation in patients with COPD. Respir Med 1999; 93: 202–207.
5) Marin JM et al. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea. The overlap syndrome. Am J Respir Crit Care Med 2010; 182: 325-331


