Wayne State University- Detroit Medical Center
Detroit, MI
Program Director: James Rowley, MD
Type of Program: Pulmonary and Critical Care Medicine
Abstract Authors: Abdulghani Sankari, MD; Sarah Lee, MD; and James Rowley, MD
BACKGROUND
Central venous catheter (CVC) placement is one of the most common procedures used for critical care management. In academic medical centers, CVC are mainly placed by trainees, making CVC training highly important for pulmonary and critical care fellows to reduce errors and complications [1]. In order to improve CVC placement education for our trainees, we started training all fellows on CVC placement using Northwestern University’s simulation-based mastery learning program [2]. The curriculum goal was to increase placement effectiveness and reduce error rates. In addition, the program included metrics to measure improvement in skills and adherence to standard practice over time using simulation techniques with ultrasound.
METHODS
Two faculty trainers were responsible for training all staff and trainees at Wayne State University/ and Detroit Medical Center (WSU/DMC) PCCM fellowship program. Each trainee underwent baseline CVC placement (both internal jugular and subclavian) knowledge assessment then watched 8 video modules on anatomic landmarks and Ultrasound techniques. The trainees were administered a 20-question written evaluation followed by a deliberate training in one-on-one sessions using a high fidelity simulation manikin and standardized clinical scenarios. For the final practical test, each trainee independently performed CVC placement, which was assessed using a checklist of 28 items (table 2). The test was followed by a debrief session on performance in the CVC placement. Outcome: The performance was considered successful (pass) if score >80% or ≤5 from 28 points were missed on the checklist.
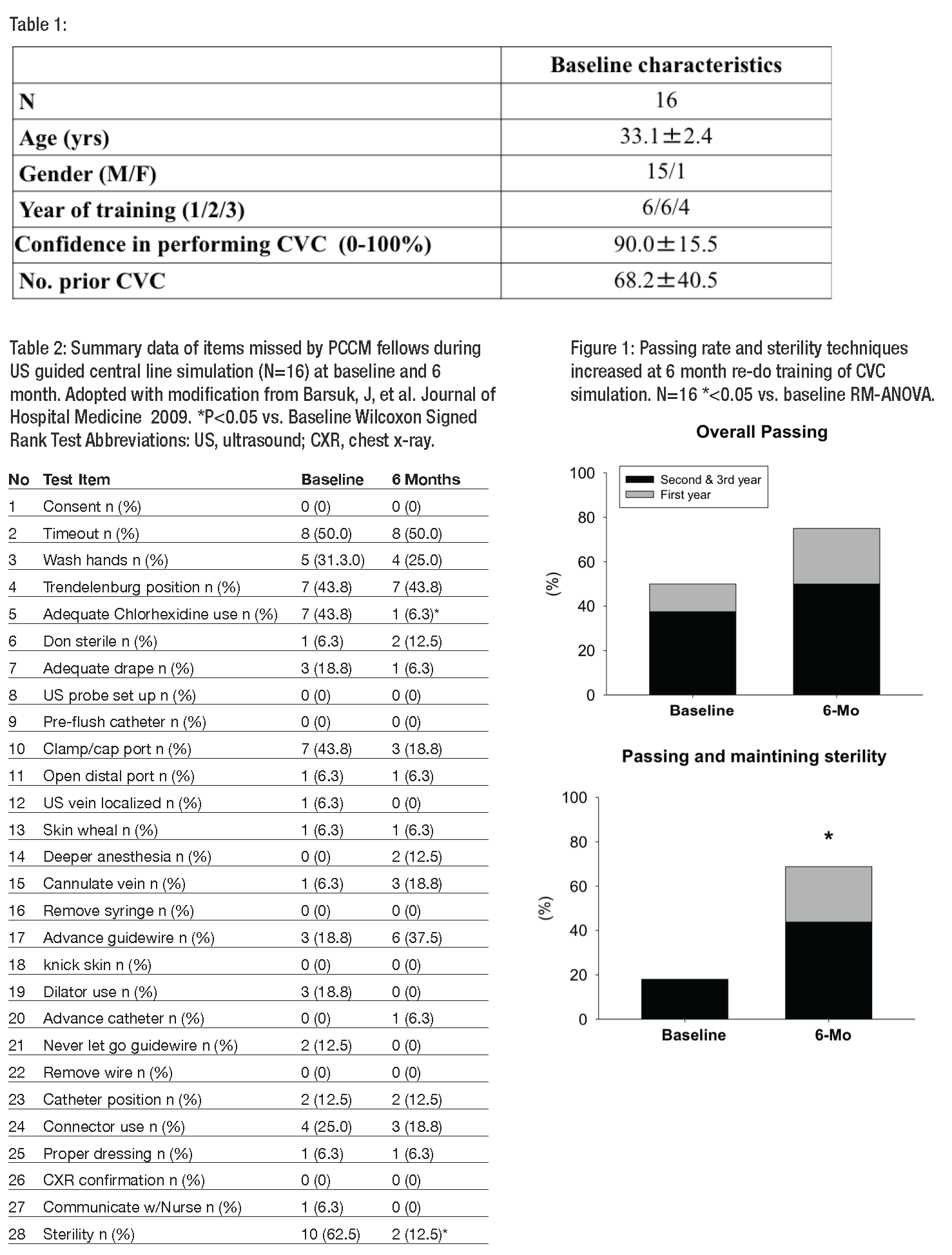
RESULTS
Since March 1, 2015, all 16 fellows have completed the program (Table 1). Of these, 12 passed the CVC training practical test and 4 failed. Despite the simulation training, significant number of trainees did not follow standard sterility techniques at baseline (62.5 percent), missed timeout procedure (50 percent), or incorrectly positioned patients (43.8 percent) on the final test. The passing rate and sterility techniques increased at 6 month re-do training of CVC simulation (Figure 1).
CONCLUSIONS
Simulation-based learning for CVC placement can be used in training fellows at different stages of their training to probe strength and weaknesses. Years of fellowship training do not affect overall scores of performance of CVC placement or passing rate. The CVC placement and sterility using simulation mastery program improve at six months compared to baseline, hence follow up training is important to achieve and maintain high level of performance.
Acknowledgment: The authors thank the simulation center at Detroit VA Medical Center for supporting this training.
REFERENCES
- Barsuk, Jeffrey H., et al. “Use of simulation-based education to reduce catheter-related bloodstream infections.” Archives of internal medicine 169.15 (2009): 1420-1423.
- Barsuk, Jeffrey H., et al. “Simulation-based mastery learning reduces complications during central venous catheter insertion in a medical intensive care unit*.” Critical care medicine 37.10 (2009): 2697-2701.