
Bilateral empyema in an immunocompromised patient
Christina Alexopoulou, MDEvangelia Akoumianaki, MD
Dimitrios Georgopoulos, MD
Department of Intensive Care Medicine, University Hospital of Heraklion, Crete Greece
Case Presentation
A 19-year-old male, with a medical history of acne treated with isotretinoine presented to the emergency department complaining of fever, sore throat, shortness of breath and pleuritic chest pain. The patient sought evaluation twenty days earlier for sore throat and fever. At that time, he was diagnosed with infectious mononucleosis and he received no pharmaceutical treatment.
Physical examination:
Vital signs revealed a temperature of 390C, HR=125/min, RR=30/min, BP=110/60 mmHg, with an oxygen saturation of 92% while breathing 100% oxygen via non-rebreather mask. The clinical examination was notable for cervical lymphadenopathy, diminished breath sounds in the lower lung fields, more prominent on the right site, and enlargement of the liver and spleen.
The patient was admitted to the ICU for further management.
Laboratory findings:
- WBC 10 620/mm3
- Hematocrit 38.4 %
- Platelets 279 000/mm3
- AST 32 units/L
- ALT 16 units/L
- Alkaline phosphatase 58 units/L
- Total bilirubin 0.99 mg/dL
- Total protein 5.6 gm/dl
- Albumin 4.1 gm/dL
- Na 150 mEq/L
- K 4.26 mEq/L
- Urea: 55 mg/dl
- Cr 0.97 mg/dL
- Serum glucose 145 mg/dL
- CRP: 32.49 mg/dl
ECG: Sinus tachycardia, ST elevation V1-V6.

The initial chest x-ray (Figure 1) revealed bilateral infiltrates with bilateral pleural effusions, larger on the right side.
ICU and hospital course:
The patient was empirically treated with levofloxacin, piperacillin/tazobactam and linezolid for presumed pneumonia. Bilateral thoracenteses were performed. Pleural fluid analysis of the purulent R-sided effusion revealed pH 6.58, LDH: 4500 U/lit. Pleural fluid analysis of the purulent L-sided effusion revealed pH 6.50, LDH: 6200 U/lit. Gram stain: negative. Chest tubes were placed bilaterally.
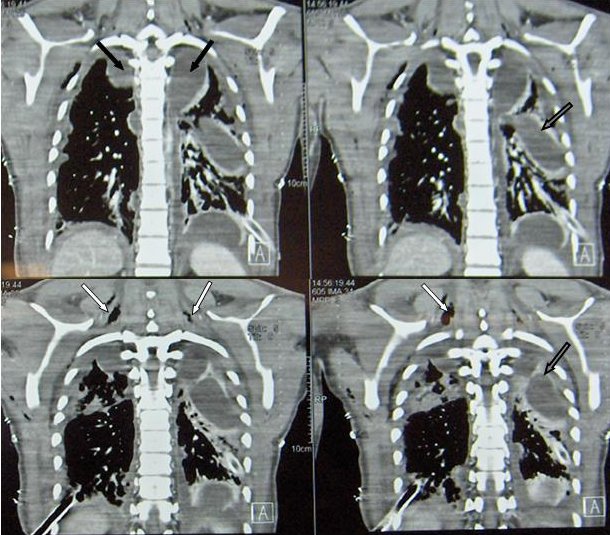
Despite the above management, the patient’s condition rapidly deteriorated, and he required endotracheal intubation and mechanical ventilation. Pain and swelling in the neck developed and a CT scan of the neck and thorax (Figure 2) demonstrated multiple cervical (white arrows) and mediastinal abscesses (black arrows) as well as bilateral empyema, (open arrows) leading to the diagnosis of descending necrotizing mediastinitis.
Treatment included radical surgical debridement of the neck and mediastinum with drainage, excision of necrotic tissue, decortication and irrigation. The cervical debridement was repeated three times. Daily irrigations of the pharyngeal and pleural spaces were performed.
Other laboratory data:
Pleural fluid cultures positive for Gemella morbillorum
Neck pus cultures positive for Streptococcus salivarious
EBV IgM + (1/40)
Due to severe septic shock and prolonged mechanical ventilation, a tracheostomy was performed. Two weeks later, the patient was hemodynamically stable and able to breathe without mechanical assistance, but after an episode of aspiration, a nasogastric tube was placed again.
He was transferred from ICU to the ENT floor on the 30th hospital day and was discharged home 2 months later with a nasogastric tube in place due to facilitate enteral nutrition in the setting of persistent swallowing difficulties, which resolved completely over the following months.
One year later the patient was completely healthy and free of any symptoms from the upper and lower respiratory system.
Question 1
What is the most common cause of bilateral empyema?
- Community acquired pneumonia
- Acute mediastinitis
- Rheumatoid arthritis
- Thoracentesis
- Malignancy
Answer to Question 1
Correct answer: B
Bilateral empyema is basically limited to conditions leading to acute bacterial mediastinitis, such as esophageal rupture, trauma and infections arising in the neck or teeth and gums, with spread of anaerobic bacteria to the mediastinum.1 Community acquired pneumonia, thoracentesis, malignancy and rheumatoid arthritis are well known causes of unilateral empyema but rarely bilateral empyema, especially in immunocompetent patients.
Question 2
What is the appropriate therapy for pleural empyema?
- Drainage, antibiotic therapy and surgery when there is no response.
- Antibiotic therapy and, if there is no response, drainage.
- No treatment until the results of cultures.
- Urokinase/streptokinase in the pleural space.
- Thoracentesis to remove the pleural fluid.
Answer to Question 2
Correct answer: A
Frank pus in pleural cavity is termed empyema and requires immediate drainage in addition to antibiotics. If the pleural fluid is not purulent, placement of a chest tube should be performed when one or more of the following criteria are fulfilled:
- pH < 7.2
- Positive Gram stain or presence of organisms on pleural fluid cultures.
- In the absence of pH measurement, pleural fluid glucose < 40 mg/dl and/or LDH > 1000 IU/Lt are suggestive of complicated parapneumonic effusion.2
Delay in chest tube drainage of the pleural space is associated with increased morbidity and duration of hospital stay and may lead to increased mortality.
When cultures do not reveal a causative organism, antibiotics should be chosen to cover organisms likely to cause pleural infections and where possible should be modified according to the results of pleural fluid culture and sensitivities. In community acquired, culture-negative pleural infection, the British Thoracic Society (BTS) suggests intravenous antibiotic regimens including:
- cefuroxime plus metronidazole or,
- benzylpenicillin plus ciprofloxacin,
- or meropenem plus metronidazole.
Hospital acquired culture negative pleural infections require broader spectrum antibiotic regimens:
- piperacillin/tazobactam or,
- ceftazidime, or
- meropenem plus metronidazole.
The use of intrapleural fibrinolytic agents remains controversial. A recent Cochrane Database review suggests that there may be some benefit, but high quality clinical studies are lacking.3 Patients should be considered for surgical treatment if they have persistent sepsis in association with a persistent empyema, despite chest tube drainage and antibiotics.4
Question 3
Which is correct regarding infectious mononucleosis (IM)?
- Empyema and mediastinitis following IM are common.
- IM usually affects immunocompromised patients.
- IgM and IgG antibodies directed against the Epstein-Barr viral capsid antigen are specific but not sensitive markers of IM infection.
- IM is a severe illness requiring hospital admission.
- IM may cause bilateral empyema through the initial development of a pharyngeal abscess.
Answer to Question 3
Correct answer: E
Infectious mononucleosis is a self-limited illness, caused by the Epstein-Barr virus (EBV), usually affecting previously healthy young people. It is characterized by a triad of fever, tonsillar pharyngitis, and lymphadenopathy. EBV is a widely disseminated herpes virus that is spread by intimate contact between susceptible persons and EBV shedders.5 EBV-induced IM should be suspected when an adolescent or young adult complains of sore throat, fever, and malaise and has lymphadenopathy and pharyngitis on physical examination. Supportive evidence of EBV infection is derived from the peripheral blood smear and a heterophile antibody test. Occasionally, EBV-specific antibodies are warranted. IgM and IgG antibodies directed against viral capsid antigen have high sensitivity and specificity for the diagnosis of IM (97 and 94 percent, respectively).
Respiratory complications of infectious mononucleosis are uncommon. They include upper airway obstruction from tonsillar enlargement or a pharyngeal abscess, bilateral hilar adenopathy, exudative pleural effusions, interstitial pneumonitis, superimposed bacterial pneumonia and septic thrombophlebitis with its consequences. A patient can develop bilateral anaerobic empyema as complication of infectious mononucleosis through two potential mechanisms, both requiring the initial development of a pharyngeal abscess. Patients can develop septic thrombophlebitis of the jugular veins resulting in septic emboli (LeMierre’s syndrome) or the abscess can invade the space between the alar and the prevertebral fasciae of the neck into a space known as “the danger space”. Once an infection enters this danger space, it has direct access into the mediastinum, resulting in mediastinitis.6 Only 2 cases of EBV-related descending necrotizing mediastinitis have been reported in the literature.6,7
Question 4
What are the diagnostic criteria of descending necrotizing mediastinitis?
- Severe oropharyngeal infection, roentgenographic features of mediastinitis, necrotizing mediastinal infection at operation or at postmortem and relationship between mediastinitis and oropharyngeal infection.
- Bilateral empyema in the absence of pneumonia.
- Severe oropharyngeal infection and pus in the mediastinum.
- Fever, dyspnea, chest pain and pharyngeal abscess.
Answer to Question 4
Correct answer: A
Mediastinitis is the inflammation of the connective tissue that lines the mediastinal structures and fills the interpleural spaces. Depending on the etiology, infectious or non-infectious, it can be acute or chronic. In its acute form, it is a life threatening condition if not diagnosed early and treated adequately.
Infectious causes of mediastinitis include mediastinal extension of pulmonary infections and head and neck infections, most commonly odontogenic infections or retropharyngeal abscesses. Other causes include peritonsillar abscesses, cervical lymphadenitis, clavicular osteomyelitis and, rarely, parotitis and thyroiditis. Non infectious causes include cardiothoracic surgery, esophageal or tracheobronchial perforation, traumatic endotracheal intubation, external trauma and intravenous drug abuse.
Descending mediastinitis involves the cervical or oropharyngeal region and is characterized by an acute, typically polymicrobial infection associated with extensive fascial necrosis that spreads towards the skin and underlying muscles. It is an uncommon form of mediastinitis that may rapidly progress to sepsis.8 A characteristic feature is its dramatically extensive character, causing severe systemic toxicity. Mediastinal abscesses commonly coexist. Other described severe complications include cranial nerve deficits, upper airway obstruction, acute respiratory distress syndrome (ARDS), pleural empyema, cardiac tamponade, erosion of the aorta, aortic aneurysm, costal osteomyelitis and rupture of the innominate artery.9
Regardless of cause, descending mediastinitis tends to affect young males, with a mean age of 36 years. Factors predicting a poor prognosis include advanced age, diabetes mellitus, alcoholism, neoplastic disease, malnutrition, poor oral hygiene and immunosuppressive conditions.
The causative organisms vary depending upon the origin of the infection. In the majority of cases it is a mixed aerobic and anaerobic infection. The following bacteria are most commonly identified: Streptococcus viridans species, coagulase negative staphylococci, Staphylococcus aureus, Bacteroides species, Peptostreptococcus species, Prevotella species, Fusobacterium species, Actinomyces species, Klebsiella pneumoniae, Haemophilus influenzae, Gemella morbillorum, Candida albicans, and Aspergillus species.10
The criteria for diagnosis of descending necrotizing mediastinitis, defined by Estrera and colleagues, include:
- clinical manifestation of severe oropharyngeal infection;
- demonstration of characteristic roentgenographic features;
- documentation of mediastinitis at operation, postmortem examination or both, and
- establishment of relation between oropharyngeal infection and development of the necrotizing process in the mediastinum.11
The diagnosis of descending necrotizing mediastinitis is suspected based on the patient history and clinical examination. Contrast-enhanced CT scan of the neck and thorax are the diagnostic tests of choice for confirmation. CT features of descending necrotizing mediastinitis include: increased density of the adipose tissues, myositis, cervical lymphadenopathy, mediastinal fluid collection (with or without gas), pleural or pericardial fluid collections and vascular thrombosis.12
Endo et al classified descending mediastinitis as either focal or diffuse, according to the degree of dissemination demonstrated by CT scan. In type I (focal type), the infection is located in the superior mediastinal space above the tracheal bifurcation. In type II (diffuse type), there are two subtypes. In subtype IIA, infection is still located in the inferior anterior mediastinum; in subtype IIB, the infectious process has reached the inferior posterior mediastinum.13
Question 5
What is the appropriate management of descending necrotizing mediastinitis?
- Antibiotic therapy
- Surgery
- Drainage with tubes
- Antibiotic therapy and aggressive surgical drainage at the time of diagnosis
- Antibiotic therapy and aspiration of pus from the abscesses.
Answer to Question 5
Correct answer: D
Descending necrotizing mediastinitis is lethal if not treated adequately and promptly. Adequate drainage and debridement, appropriate antibiotic therapy, and sufficient nutritional and respiratory support are the main elements of treatment. However, the mainstay of treatment is surgical excision and drainage of necrotic tissues. There are several surgical options depending on the site, extent of infection and surgical experience.
Generally, the choice between external and intraoral approach depends on the site of the abscess, its anatomical relationship with the great vessels, and the extent of mediastinal necrosis. If only the upper mediastinum above the carina is involved, mediastinal transcervical drainage is sufficient. However, in extensive necrosis, mediastinal transcervical drainage should be associated with right posterolateral thoracotomy for better outcome. Estrera et al established that if the descending mediastinitis extends below the tracheal bifurcation anteriorly or at the level of the fourth thoracic vertebra posteriorly, mediastinal drainage should be associated with a transthoracic approach.14 Other options include the transthoracic approach, either using clamshell or subxiphoid incision and median sternotomy. Endo et al reviewed reported cases and concluded that mediastinal abscess above the carina can be successfully treated by the cervical approach, while thoracotomy should be performed for descending abscess located in the anterior or posterior mediastinum below the carina. Similar conclusions were drawn by Wheatley and Marty et al.13,15,16 Abscesses tend to re-form in the days after surgery, and a daily irrigation and drainage of the mediastinum and cervix are helpful in preventing abscesses from re-forming.
Surgical options for descending necrotizing mediastinitis17
|
Transcervical |
Posterolateral thoracotomy |
Median sternotomy |
Transthoracic |
|
Descending Mediastinitis type I |
Descending Mediastinitis type IIA and IIB |
Good view of the operative field |
Use of clamshell incision or subxiphoid approach |
|
Less invasive |
Easily access to all |
Can be performed in cases of bilateral infections |
Clamshell incision: excellent exposure of all mediastinal structures. |
|
May not reach deep regions |
Allows pulmonary decortication |
Risk of sternal osteomyelitis and dehiscence |
Clamshell incision is very invasive and carries the risk of damaging the phrenic nerve. |
Question 6
What is the mortality rate of descending necrotizing mediastinitis?
A. 80%
B. 20%
C. 40%
D. 60%
E. 90%
Answer to Question 6
Correct answer: C
Despite early diagnosis, effective antibiotics and aggressive surgical treatment, the mortality of descending necrotizing mediastinitis patients remains as high as 40% to 50% due to the persistence of infection with empyema, pericarditis and blood vessel erosion.11 Late diagnosis and delayed or inappropriate treatment are the main determinants of high mortality. Other factors contributing to poor prognosis include the severity of infection and the patient’s underlying comorbidities. The causes of death are multiple: septic shock and multiple organ failure, airway obstruction, cardiac tamponade, ARDS, gastrointestinal haemorrhage. Early utilization of CT for the diagnosis of descending necrotizing mediastinitis and aggressive surgical management using thoracotomy reduced the mortality rate to 14% in a series of seven patients as reported by Sancho Melero et al.15
In conclusion, rapid diagnosis based on high index of suspicion leading to contrast-enhanced CT imaging of the cervix and thorax, aggressive early surgical management, broad antibiotic coverage and careful postoperative wound management can salvage a patient with this highly fatal disease.
REFERENCES
- Alsoub H, Chacko KC. Descending necrotising mediastinitis. Postgrad Med J 1995; 71: 98-101.
- Light W. Richard and Gary Lee Y.C. Textbook of Pleural Diseases 2003.
- Cameron R, Davies HR. Intra-pleural fibrinolytic therapy versus conservative management in the treatment of adult parapneumonic effusions and empyema. Cochrane Database Syst Rev 2008 Apr 16;(2):CD002312.
- Davies C W H, Gleeson FV, O Davies RJ. BTS guidelines for the management of pleural infection. Thorax 2003; 58 (Suppl II): ii18-ii28.
- Evans AS, Niederman JC, Cenabre, LC, West B, Richards VA. A prospective evaluation of eterophile and Epstein-Barr virus-specific IgM antibody tests in clinical and subclinical infectious mononucleosis: Specificity and sensitivity of the tests and persistence of antibody. J Infect Dis 1975; 132:546.
- Andrianakis I, Kotanidou AN, Marinos T. Pitaridis G, Saroglou J, Exarhos DN, S. Roussos CS, Bellenis IP. Life-threatening bilateral empyema and mediastinitis complicating infectious mononucleosis. Intensive CareMed 2002; 28: 663-664.
- Irwin R, Mello C, Umali C. Bilateral anaerobic empyema complicating infectious mononucleosis. Chest 1997; 112:833–835.
- Cirino LM, Elias FM, Almeida JL. Descending mediastinitos: a review. Sao Paulo Med J. 2006; 124(5) : 285-90.
- Brunelli A, Sabbatini A, Catalini G, Fianchini A. Descending necrotizing mediastinitis. Arch Otolaryngol Head Neck Surg 1996; 122:1326-9.
- Boscolo-Rizzo P, Marchiori C, Montolli F, Vaglia A, Da Mosto MC.Deep Neck Infections: A Constant Challenge. ORL 2006; 68: 259-265.
- Estrera AS, Landay MJ, Grisham JM, Sinn DP, Platt MR. Descending necrotizing mediastinitis. Surg Gynecol Obstet. 1983; 157:545-52.
- Scaglione M, Pinto A, Giovine S, Di Nuzzo L, Giuliano V, Romano L. CT features of descending necrotizing mediastinitis – a pictorial essay. Emerg Radiol 2007; 14: 77-81.
- Endo S, Murayama F, Hasegawa T, Yamamoto S, Yamaguchi T, Sohara Y, Fuse K, Miyata M, Nishino H. Guideline of surgical management based on diffusion of descending necrotizing mediastinitis. Jpn J Thorac Cardiovasc Surg 1999; 47:14–19.
- Sancho LM, Minamoto H, Fernandez A, Sennes LU, Jatene FB. Descending necrotizing mediastinitis: a retrospective surgical experience. European Journal of Cardiothoracic Surgery 1999; 16, 200-205.
- Marty-Ane CH, Alauzen M, Alric P, Serres-Cousine O, Mary H Descending necrotizing mediastinitis – advance of mediastinal drainage with thoracotomy. J Thorac Cardiovasc Surg 1994; 107: 55–61.
- Wheatley MJ, Stirling MC, Kirsh MM, Gago O, Orringer MB. Necrotizing mediastinitis – transcervical drainage is not enough. Ann Thorac Surg 1990; 49: 780–784.
- Lavini C, Natali P, Morandi U, Dallari S, Bergamini G. Descending necrotizing mediastinitis. Diagnosis and surgical treatment. J Cardiov Surg (Torino) 2003; 44 (5): 655-60.


